NEONATAL APNEA
I. Definition
A. Short (< 10 secs) breathing pauses can be normal at all gestational ages.
B. Clinical apnea (leading to physical intervention) is CURRENTLY defined as:
1. apnea > 20 seconds in infants > 40 weeks post menstrual age or
2. any apnea when accompanied by bradycardia (<100 bpm in preterm infants, < 80 bpm in term infants). Almost always accompanied by oxygen desaturations < 85% in infants < 32 weeks PMA or < 90% in infants > 32 weeks PMA).
C. Apnea can be central, obstructive or mixed in origin.
II. Incidence
A. 25% of all infant < 34 weeks of gestation (~1800 grams).
B. Almost all infants < 30 weeks gestation
C. Apnea of prematurity (AOP) usually begins at 1-2 days of life, peaks around 7 days of life and is rarely associated with new onset after 7-10 days of age (without other complicating or precipitating events). It may persist for a few weeks beyond 40 weeks post-menstrual age in preterm infants < 28 weeks gestation at birth. General anesthesia can result in acute exacerbation of apnea of prematurity post operatively (generally resolves within 24 hours).
III. Pathogenesis
A. Apnea of prematurity
1. apnea associated with oscillatory breathing (periodic breathing)
2. immature chemoreceptor function
3. respiratory center depression (drugs, asphyxia, hypoxia)
4. breathing highly dependent on cortical activity (sleep state)
5. heightened (immature) pulmonary reflexes
6. upper airway (obstruction due to activation of laryngeal chemo/mechano receptors or incoordination of upper and lower airway muscle contractions particularly the tongue).
7. Chest wall excursion restriction
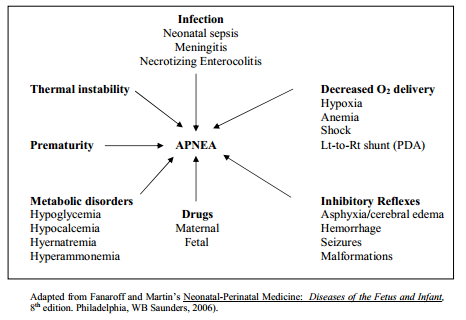
B. Other Causes of Apnea (be particularly suspicious in the more mature infant, but consider after the first apnea in any baby).
1. acute respiratory disease - also associated with hypoxia and acidosis.
2. metabolic disturbances - hyper/hypoglycemia, hyper/hyponatremia, hypocalcemia, azotemia, hyperammonemia.
3. infection (apnea frequently presents as a subtle presentation of late onset nosocomial infections)
4. rapid warming - particularly in an incubator
5. CNS - residual from asphyxia, ischemia, IVH, seizures
6. severe anemia
7. congenital heart disease - PDA causing pulmonary edema is most common
8. gastrointestinal reflux (see enteral nutrition chapter).
9. Hypothermia
10. Maternal drug exposure (i.e., magnesium sulfate exposure)
IV. Monitoring and Evaluation
A. All infants should be monitored on admission to the NICU
B. Infants < 34 weeks (< 1800 gms) should be monitored with a cardiorespiratory monitor until clinically apnea-free for 5-10 days or until hospital discharge.
C. Any baby with a recent history of apnea should be monitored.
D. After the first apnea, consider an evaluation for other possible causes. Work up might include a rule out sepsis evaluation, evaluation of glucose, calcium or sodium imbalance, hematocrit, blood gases, and chest X-ray. Also check the nursing flow sheet for rapid changes in incubator temperature that may have been associated with apnea events.
V. Treatment
A. Who should be treated? Infants with apnea requiring intervention such as stimulation, bagging, etc. and occurring more than 3-6 times per day or several episodes per hour should be treated. Not all patients with apnea need to be given medication.
B. Mild apnea may respond to correcting mild hypoxia with nasal cannula oxygen (saturations need not exceed 95%)
C. Severe Apnea:
1. Xanthines - see Chapter 7 for doses. Our drug of choice is almost always Caffeine citrate, either intravenously or orally (20mg/kg loading dose followed by 5 mg/kg daily maintenance dosing). Drug monitoring is rarely needed unless either no effect is noted or if an infant exhibits signs and symptoms of caffeine toxicity (usual therapeutic effects are seen with blood levels of 15-30 mg/dL).
2. Because of the long half-life of caffeine, a change to caffeine requires at least an 8-12 hour delay from the last Aminophylline/Theophylline dose (if this drug has been previously used).
3. Nasal CPAP may also be effective, particularly in the small baby (primarily assists by blowing the tongue and other upper airway soft tissues out of the path of the upper airway). CPAP may also improve oxygenation by increasing FRC, and aid in recruiting CNS stimulation by resetting Herring-Bruer stretch reflex in lungs).
VI. Persistent Apnea
A. Occasionally, infants will continue to have apnea as they approach term and are ready for discharge.
B. A re-evaluation may be indicated to rule out other causes such as GE reflux (most commonly associated with severe recurrent bradycardia) or CNS-related problems.
C. A hardcopy 12-24 hour multichannel study (esophageal pH or manometry, HR, RR, O2 sats and nasal obstruction probe) may be helpful in quantitating the number of events and correlating any unusual interrelationships (for example, a lot of desaturations and periodic breathing in the presence of frequent esophageal pH drops may indicate that reflux is a problem). Multichannel studies can be ordered following discussion with the Attending.
D. Occasionally an infant is ready to go home except for the presence of brief, self-correcting apnea and/or bradycardia spells. In this case, discuss potential home monitoring with an Attending physician. The parents should be made aware of these plans as far ahead as possible as they will need home monitor training and CPR training (also to be ordered and arranged as far in advance as possible).
VII. Going Home
GUIDELINES FOR WITHDRAWAL OF XANTHINES AND DISCHARGE OF INFANTS WITHOUT HOME MONITORING.
Eligibility for xanthine discontinuation :
Any infant with a current weight > 1250 grams
Stable without need for CPAP or upward adjustment in xanthine dosing for 7 days or more
Infant has not had any significant apnea ( Significant apnea defined as respiratory pause > 20 seconds or any apnea associated with a bradycardia < 80 bpm for > 10 seconds or desaturations of < 85% ) requiring physical stimulation or positive pressure ventilation in the prior 7 days. These 7 days of non-significant AOP must be documented in the nursing log and/or with electronic documentation via the cardiorespiratory monitor.
Bradycardia associated with oral feeding is not pathological and does not require xanthine therapy or monitoring.
Eligibility for monitor discontinuation :
Once an infant meets xanthine discontinuation eligibility requirements, the xanthines may be stopped.
Following an additional 10 days of non-significant apnea and bradycardia, an infant may be considered to be at very little risk of additional AOP events and can be safely discharged to home without a home apnea monitor. These 10 days of additional non-significant AOP must be documented in the nursing log and/or with electronic documentation (if available).
For most infants with “uncomplicated” apnea of prematurity in which the decision is made to discharge the infant to home on a home apnea monitor ( + xanthine therapy), the duration of home monitoring and xanthine therapy should generally not exceed 4-8 weeks beyond the mother’s due date. A hard copy download of events from the “smart” version of these home monitors is often reassuring for the parents and the primary physician prior to discontinuation of the monitor.
The physician caring for the infant following discharge should be aware of infants going home on monitors and what the plans are for any anti-apnea meds and monitor alarm parameters and duration of use.
The parents should be instructed that the home monitor should only be utilized during those periods of time that the infant is not being directly observed by a competent care provider, i.e., sleeping at night, infant in a separate part of the house, infant in car seat. The home monitor should NOT be utilized during feeds. The majority of recorded alarms that are interpreted by physicians or other trained personnel are due to artifact related events. If infants are at home on continuous monitoring, the number of alarms (and associated artifact related events) increases, potentially frustrating the parents and making determination of real pathology more difficult for the interpreters.
Any infant being discharged on a monitor should be admitted to the Apnea program (The Respiratory Therapy personnel) to insure good follow-up and provide parent and local Pediatrician support.
Nursing Descriptors of Apnea/Bradycardia/Desaturation Events (for use in daily flow sheet charting)
Activity Level Descriptors: Quiet, Asleep, Drowsy, Crying, Lethargic, Floppy, Feeding
Color Change : Pale, Dusky, Mottled, Cyanotic, No change
Apnea : no breathing for > 15 seconds in a premature infant < 38 weeks PMA or > 20 seconds in a term infant
Bradycardia : heart rate < 100 bpm for > 10 seconds in a premature infant < 38 weeks PMA or < 80 bpm for > 10 seconds in a term infant
Stimulation :
- Self: no intervention required. Event lasts < 10 seconds
- Mild: requires tactile stimulation < 20 seconds or extra oxygen for < 1 minute
- Moderate: requires stimulation > 20 seconds but < 40 seconds or extra oxygen > 1 minute*
- Vigorous: Bag-mask ventilation needed or a call is required for additional assistance*
* Moderate and Vigorous adjectives ALWAYS REQUIRE A WRITTEN DESCRIPTION OF THE EVENT!
