Intubation
Indications: To provide airway for mechanical respiratory support
Equipment:
Technique:
Equipment:
- Laryngoscope/straight blades
- No. 00 for babies <1000g
- No. 0 for babies 1-3kg
- No. 1 for babies >3kg
- ET tube of appropriate size
- suction catheters #8, #10 / suction apparatus
- Neopuff or bag & mask, oxygen
- gloves, scissors, tape
Technique:
- Extend infant’s neck slightly – avoid hyperextension; consider roll of line to support shoulders)
- Clear oropharynx / empty stomach with gentle suctioning (esp. if BMV >2min)
- Ventilate with Neopuff or bag & mask before starting, if necessary
- Hold laryngoscope in left hand, open infant’s mouth & move tongue with right forefinger
- Insert laryngoscope blade in midline; advance until its tip is between base of tongue & epiglottis within vallecula, position blade to visualize glottis
- Suction if necessary
- Hold tube with concave curve anterior, pass down right side of mouth (outside the blade) through the cords approximately 2cm into trachea
- Stop procedure to ventilate with bag & mask anytime heart rate drops below 100 or if the infant becomes cyanotic
- Check correct placement with CO2 detector à color change from purple to yellow with correct placement
- After intubation, listen for breath sounds in both lungs and over stomach
- In general, correct placement is: birthweight + 6
- Secure tube
- Confirm appropriate tube placement with CXR
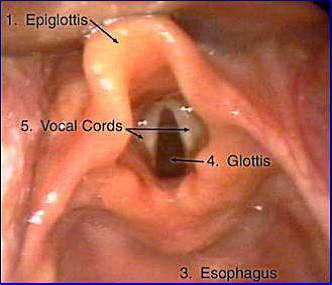
Representation of view of larynx during direct laryngoscopy.
Lumbar Puncture
INDICATION: to obtain specimen of CSF for exam and culture
EQUIPMENT:
COMPLICATIONS:
EQUIPMENT:
- LP tray - use 25g Neonatal LP needle
- sterile gloves, mask, cap
- Position infant on side with back rounded, parallel to table or sitting with back rounded and perpendicular to table
- Cleanse area 3 times with betadine beginning at desired interspace & wash with enlarging circles to include iliac crest
- Drape
- Insert needle into 3rd or 4th lumbar interspace at level of top of iliac crest aiming slightly cephalad
- Advance needle slowly to a depth of 1-1.5cm in term newborn, less in preemie
- Remove stylet frequently to check for fluid – it is ok to remove stylet after needle is through the skin and just manipulate the needle
- Collect ½ - 1ml of CSF in each of 3 tubes
- Replace stylet and remove needle
- Apply gentle pressure until fluid stops leaking
- Send CSF for the following:
- Tube #1 – gram stain, culture and sensitivities, meningitis PCR
- Tube #2 – protein and glucose
- Tube #3 – cell count and differential
- Tube #4 – any additional studies (HSV PCR)
COMPLICATIONS:
- Hypoxemia from positioning / aspiration
- Bleeding
- Infection
- Damage to surrounding structures
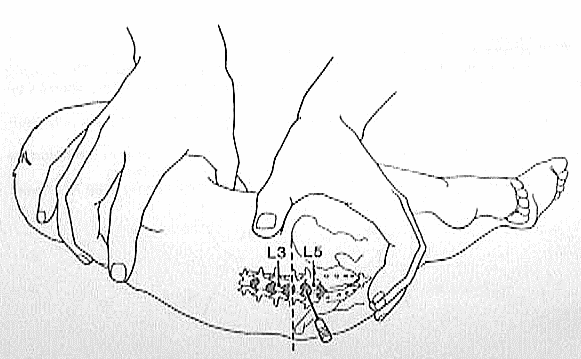
Positioning landmarks used for lumbar puncture. The iliac crest (dotted line) marks the approximate level of L4
Umbilical Vessel Catheterization
Indications:
Equipment
Technique:
Complications:
- Umbilical Artery Catheterization
- Monitoring of arterial blood gasses and/or direct BP monitoring
- Umbilical Venous Catheterization
- Resuscitation
- To monitor central venous pressure
- Access when peripheral IV cannot be placed
Equipment
- Sterile gloves, gown, mask, cap
- Cloroprep for infants > 29 weeks or betadine for infants < 29 weeks
- Umbilical catheter tray
- Umbilical catheters
- 3.5F for < 1200g
- 5.0F for > 1200 - 1500g
- 3.5F for < 1200g
- Infusion pump with appropriate IV solution
- Sterile saline + heparin or premixed heparin solution
- 3-way stop cock with Luer-lok
- Restraints
- Radiant warmer
Technique:
- Restrain neonate
- Prepare catheters
- Place stopcock at each lumen and flush each port with saline solution
- Place stopcock at each lumen and flush each port with saline solution
- Prep cord with chloroprep/betadine
- Assistant can hold the cord clamp
- Assistant can hold the cord clamp
- Position sterile umbilical tape around base of cord and loosely tie
- This can be pulled tight for hemostasis should any bleeding occur
- This can be pulled tight for hemostasis should any bleeding occur
- Cut the cord horizontally across with scalpel to leave approximately 1 cm of umbilical cord above the abdomen
- A clean cut usually does bleed since the arteries spasm
- A clean cut usually does bleed since the arteries spasm
- Drape the neonate – clear drape and avoid obscuring the infant’s face
- With forceps pick up side of umbilical stump - identify 2 arteries & 1 vein
- Dilate umbilical vessel carefully with curved non-toothed Iris forceps
- Initial dilation of artery lumen is most important step since creation of false lumen will result in failure to catheterize vessel & increase risk of perforation
- Initial dilation of artery lumen is most important step since creation of false lumen will result in failure to catheterize vessel & increase risk of perforation
- Introduce catheter into vessel & advance
- never use force - gentle, constant pressure will overcome vessel spasm
- never use force - gentle, constant pressure will overcome vessel spasm
- calculate length of catheter:
- UAC: 1/3 body length + 1 cm or [bw(kg) x3] +9
- UVC: 1/3-2/3 perpendicular distance from infant’s shoulder to level of umbilicus or UAC depth/2 + 1
- Marks on catheter are every 1cm
- Remember catheter can be pulled back if it’s in too far; it CANNOT be advanced if not in far enough once sterile field is broken
- UAC: 1/3 body length + 1 cm or [bw(kg) x3] +9
- Always verify placement of catheter with XRay
- UAC: between T6-T9 if high UAC or L3-L4 if low lying
- UVC: between T8-T9 @ diaphragmsecure catheter with 4.0 silk suture
- UAC: between T6-T9 if high UAC or L3-L4 if low lying
- Secure catheter with 4.0 silk suture
Complications:
- UAC
- Malpositioned catheter - vessel perforation, peritoneal perforation, false aneurysm
- Vascular accident - thrombosis/embolism, vasospasm, hypertension
- Hemorrhage
- Infection
- NEC
- IVH
- UVC
- Air embolism
- Hemorrhage
- Infection
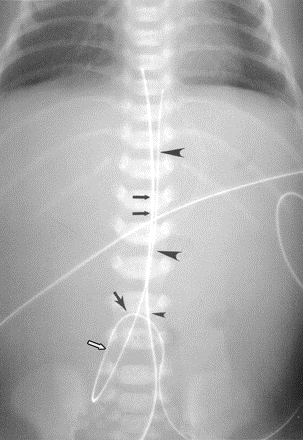
Normal radiographic appearance of UVC & UAC. Frontal radiograph of abdomen shows that UVC enters abdomen at umbilicus (small arrowhead), travels in cephalad direction in umbilical vein (double black arrows) (note that catheters cross just above umbilicus), courses through left portal UAC also enters abdomen at umbilicus (single black arrow) but extends inferiorly (white arrow) and posteriorly into iliac artery before coursing superiorly in aorta (large arrowheads).
