Central Lines
General
- Attempt to avoid all central lines if peripheral access is satisfactory. Percutaneously inserted central lines (PICCs) may be appropriate in selected infants (the very low birthweight infant or the recovering septic infant, both of whom need prolonged vascular access).
- Complications of central lines are often major (e.g., loss of foot, thrombosis of SVC, sepsis, etc.)
- Although its efficacy is controversial, we heparinize all solutions entering central lines.
- For infusions in infants < 1500 grams, 0.5 units of heparin/cc
- For infusions in infants > 1500 grams, 1.0 unit of heparin/cc
- For infusions in infants < 1500 grams, 0.5 units of heparin/cc
Umbilical Artery Catheter (UAC)
Who may need an umbilical artery catheter?
B. How to insert a UAC
DANGERS
When to Pull an Umbilical Artery Catheter
1. In general, when the inspired oxygen concentration is less than 30%, it is time to consider pulling the arterial catheter. Often, transcutaneous monitoring of oxygen saturations and an occasional capillary blood gas will suffice instead of an arterial blood gas.
2. When continuous arterial pressure monitoring is no longer required.
Technique
- Most newborn infants persistently requiring > 40% oxygen and frequent arterial blood gas sampling
- Most extremely low birth weight infants (< 1000 grams birth weight)
- Infants requiring continuous arterial blood pressure monitoring, e.g.
- Infants with respiratory distress requiring positive pressure ventilation
- Infants with pulmonary hypertension and hypoxia
- Severe asphyxia or septic shock
B. How to insert a UAC
- Sterile technique (cap, mask, gown, gloves, eye protection). Two people attempting this procedure are better than a solo individual attempt.
- 3.5 Fr catheter in infants < 1500 gms, 5.0 Fr catheter for infants > 1500 gms
- Calculate the length of the catheter: 1/3 body length + 1 cm OR [bw(kg) x3] +9
- The correct insertion position for “high” UAC placement is between T6 -T9, and although the GHS staff does not like “low” UACs (they have a propensity to fall out and put the baby at risk for acute hemorrhage or increase the risk of microemboli to the lower extremity), occasionally we receive a referred infant with one in place. It can be used with attending permission but should have its tip confirmed by X-ray to be between L3 - L4 (below the origin of the renal artery).
- UAC position must be confirmed by x-ray.
- If the UAC is too low, DO NOT PUSH IT IN FURTHER unless the field is still sterile.
- All UACs must be sutured in place. Try not to suture the umbilical skin.
- All UACs must then be further secured with a tape bridge.
DANGERS
- Large blood losses may occur if the catheter comes out or the stopcock becomes disconnected.
- Any clots or bubbles may act as emboli and cause infarction to “downstream organs;” the kidneys, the intestines, or lower extremities.
- It is well established that silastic and polyvinyl chloride catheters initiate thrombi formation around the entire length of the catheter beginning the first day after insertion. Whenever the UAC serves no - or only a minimal purpose - it should be removed.
When to Pull an Umbilical Artery Catheter
1. In general, when the inspired oxygen concentration is less than 30%, it is time to consider pulling the arterial catheter. Often, transcutaneous monitoring of oxygen saturations and an occasional capillary blood gas will suffice instead of an arterial blood gas.
2. When continuous arterial pressure monitoring is no longer required.
Technique
- Pull the catheter out slowly over a few minutes until 1 to 2 cm remain.
- When the visible pulsations stop, usually after 1 to 2 minutes, pull the catheter and apply pressure by pinching the abdominal skin below the umbilicus.
- Do not turn the catheter off and “allow the line to clot” - You are waiting for the vessel to constrict - not clot off.
Umbilical Venous Catheter (UVC)
Umbilical Venous Catheters - can be placed most easily in the first 24 hours of life but may also be placed up to 4-5 days of life (see section B3, below).
Indications for a UVC
How to Insert a UVC
Care of the UVC
Indications for a UVC
- Emergency medication, particularly in the delivery room.
- Infants < 1000 grams birthweight (or more, if acutely ill)
- Exchange transfusions
- Infants requiring central venous pressure monitoring
- those with pulmonary hypertension
- those with shock/asphyxia/sepsis
- any infant with complicated fluid and electrolyte problems may benefit from a UVC.
How to Insert a UVC
- Technique is similar to that of a UAC
- Measure catheter placement: 1/3-2/3 perpendicular distance from infant’s shoulder to level of umbilicus OR UAC depth/2 + 1
- It is usually more difficult to insert a venous catheter into the RA than it is to put in a UAC. This is because the ductus venosus closes early and the catheter will often times end up in the hepatic portal system. In general, it is easier in infants < 24 hours old or in very sick infants.
- because it is easy to inadvertently place the UVC in the liver, it is important to determine the location (X-ray) of the tip of the UVC before infusing drugs - the exception being the emergency in the DR.
- In an emergency, it is probably best to position the UVC below the liver (insert it only 2-3 cm) and hope that emergency meds pass through the ductus venosus and not the hepato-portal system.
Care of the UVC
- The external attachment to the Wharton’s jelly and to the skin around the umbilicus is the same as for a UAC
- You may infuse through a UVC if it is not in the liver and if it is above the diaphragm (but not too high). Blood, antibiotics, drugs, and hyperalimen- tation may be infused safely.
- Umbilical venous catheters are associated with an increased frequency of nosocomial infection, more so than UACs. Therefore, it is important to remove them early, as soon as there is no longer any indication. When the catheter is removed, pressure to stop bleeding is applied superior to the umbilicus.
- Do not infuse any hypertonic solutions or drugs through an umbilical venous line until you are certain of the catheter’s position.
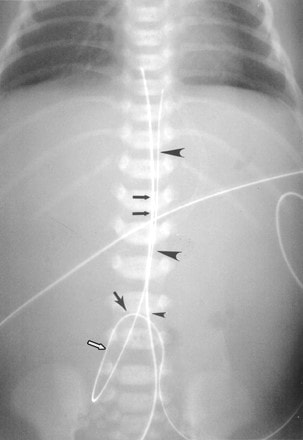
Normal radiographic appearance of UVC & UAC. Frontal radiograph of abdomen shows that UVC enters abdomen at umbilicus (small arrowhead), travels in cephalad direction in umbilical vein (double black arrows) (note that catheters cross just above umbilicus), courses through left portal UAC also enters abdomen at umbilicus (single black arrow) but extends inferiorly (white arrow) and posteriorly into iliac artery before coursing superiorly in aorta (large arrowheads).
