GENERAL GUIDELINES FOR USE OF PARENTERAL NUTRITION
I. Who is eligible?
A. Acutely ill infants for whom enteral feedings are not anticipated for 3 or more days.
B. Chronically ill infants for whom you feel the benefits of parenteral nutrition outweigh the risks.
C. Infants with gastrointestinal malformations or injury or severe malabsorption.
D. Most premature infants.
II. When?
A. On admission day if infant is stable and you anticipate a prolonged period of time (i.e., more than 4-5 days) before attaining full enteral feedings. This population would include almost all infants < 34 weeks post menstrual age.
B. Certain post-operative patients - after fluid and electrolyte management is stable.
C. Older infants with acute illness once fluid and electrolyte management are stable.
III. How?
A. Peripheral IV – preferred for short-term access but has limitations
B. Central line (usually PICC line). Central lines are usually placed for long-term intravenous access needs. They can accommodate higher osmolality concentrations of IV fluids (> 1000 mosmoles) versus peripheral IVs.
IV. What?
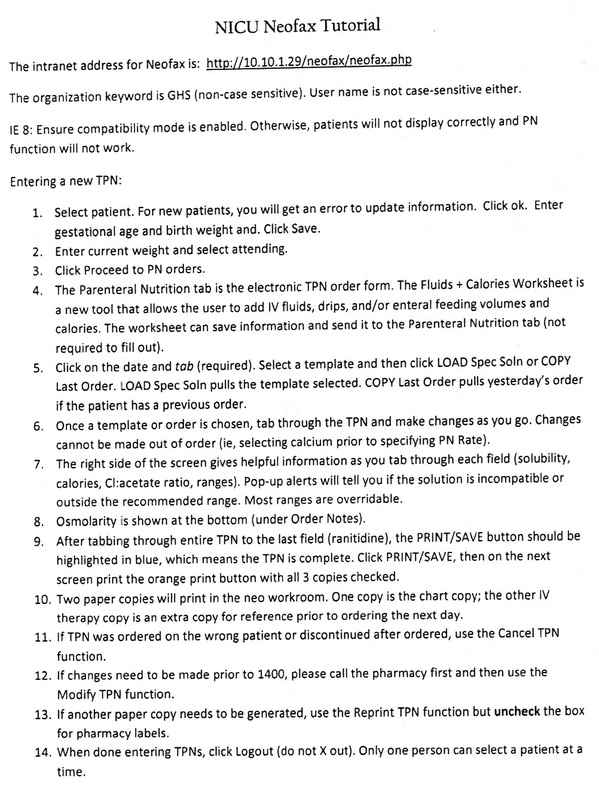
An order sheet is available in our NICU that outlines orders for glucose, protein and fat administration as well as recommended doses for electrolytes. Ideally, this order sheet must be completed for each patient needing TPN/IL by 14:00 each day. Write TPN/IL orders for infants upon admission if an infant is admitted in the morning so that TPN/IL may be begun that evening.
A. Glucose
1. Amount - up to 20 gm/kg/d (peripheral IVs limited to D12.5 or less). Infants who are fluid restricted to < 120 cc/kg/d may need higher dextrose concentrations (up to D20-25 by Central Line).
2. Method - Start with the solution that provides the gm/kg/d that is being tolerated in previous IVF and increase to maximum over several days. In a first day infant, D10 is usually tolerated well by infants > 1000 grams birth weight. Smaller infants may not tolerate this level of dextrose.
3. Adverse Effects
- hyperglycemia
- glycosuria
- osmotic diuresis
- post-infusion hypoglycemia
4. Monitor
- blood glucose is more accurate than serum glucose
- Fluid input and output (I & O)
B. Protein (as amino acid)
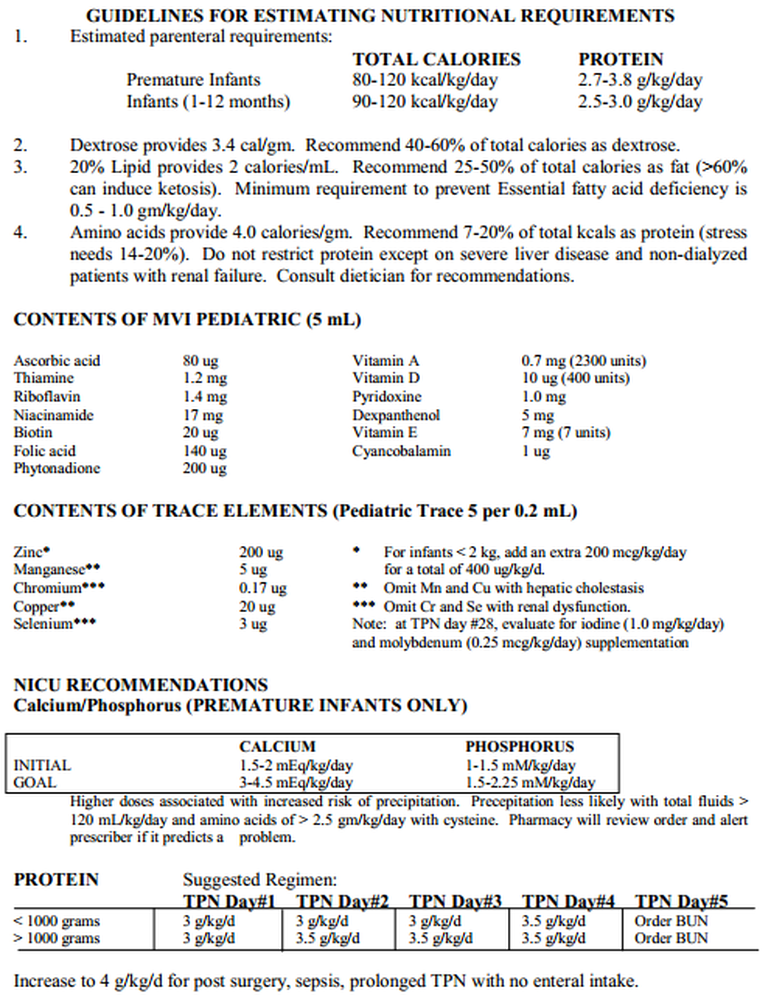
1. Amount - For normal maintenance and growth in most infants, 3-3.5 gm/kg/day of amino acids are adequate - should be 8-15% of total calories. In some rare cases, infants may require more, ( 4.0 gm/kg/day).
2. Method: start with 3.0 gm/kg/d. Increase to 3.5 gm/kg/day the following day, except in the very sickest or smallest neonates (confer with your Attending physician if you have questions). It is important to start protein ASAP in very low birth weight infants as they are highly catabolic without protein supplementation and because concomitant protein administration improves glucose tolerance.
3. Potential Adverse Effects
- azotemia (although recent studies reveal this to be unlikely)
- acidosis (seen when amino acids provide > 15% of total calories)
- serum amino acid imbalance
- hyperammonemia
- ? hepatic injury
- ? cholestasis
- ? neurological injury if > 4.0 gm/kg/day
4. Monitor
- liver function studies (every 7-10 days including GGT, SGOT, SGPT and bilirubin levels )
- ?BUN (see azotemia comments above)
- pH
5. Source - Trophamine is the amino acid formulation available for use in hyperal in the NICU.
Fat - current preparations (soy oil or safflower oil extracts) contain a high content of polyunsaturated fats (double bonds between carbon atoms). Polyunsaturated fats (PUFAs) are essential in the diet (linoleic acid, arachidonic acid, docosahexanoic acid). However, they are also predisposed to rapid decomposition into toxic lipid aldehydes and peroxides via free radical mechanisms. We suggest that for the first several days of life, infants < 750 grams receive limited concentrations of Intralipid supplementation (1 - 2 gms/kg/day of Intralipids). At 3-4 days of life, the < 750 gram infant may then be advanced to 3-3.5 gm/kg/day of Intraplipid. Monitor serum triglyceride levels prior to advancing from 2 gms/kg/day. In addition, because Intralipid components can displace bilirubin from albumin, we recommend that infants with significant risk of kernicterus (i.e., the infant < 750 gms birthweight, the infant with hemolytic anemia, or the asphyxiated infant) be cautiously advanced to maximal Intralipid concentrations.
Maximum amount - 3.0 gm/kg/day. Older, more mature infants who are fluid restricted and experiencing glucose intolerance may require up to 4 gm/kg/day. Fat calories should provide between 40-50% of total calories.
2. Method - begin with 2.0 gm/kg/day. You may advance to a maximum of 3.0 gm/kg/d. Because Intralipids have been associated with an increased risk of nosocomial infections (especially Staphylococcal infections), we recommend infusing them over 18-20 hours rather than over the entire 24 hour day. Beware that some of the smallest and/or sickest infants will not tolerate this shorter infusion intervals.
3. Adverse effects
- displaces bilirubin from albumin (at high doses)
- altered oxygen diffusion secondary to “coating” of the RBC
- altered immune function and associated with increased infections
- altered platelet function
- altered prostaglandin synthesis
- deposited in lungs, liver, spleen (lipid overload syndrome)
- polyunsaturated fats (like Intralipid) are very predisposed to oxidative insult (many investigators think intralipids should be light protected to prevent photo-oxidation)
4. Monitoring
- serum Triglyceride level weekly (should = < 200 mg/dL) or more frequently in very sick or very immature infants
- direct bilirubin weekly
- liver function studies weekly x 1 wk, then q 2 weeks.
5. The lipid dose may need to be decreased to the minimum amount to meet essential fatty acid needs (0.5 gm/kg/day) and the triglyceride level may need to be monitored more frequently in the following conditions:
- hyperbilirubinemia approaching exchange transfusion levels
- liver disease
- sepsis (acute phase)
- severe pulmonary disease
D. Electrolytes (see attached TPN order sheet)
1. These are suggestions only. Some infants will require adjustment more than once/day. Generally those infants requiring very frequent electrolyte adjustments should not be on TPN. However, if this situation is anticipated, TPN may be calculated to provide some % of total fluids and electrolytes and the remainder provided as non-amino acid containing IV fluids which may be changed more frequently and at less expense.
2. When initiating TPN, electrolytes should be monitored q day for 2-3 days and then at least once per week thereafter. Infants receiving the same TPN formulation for long periods of time may need even less monitoring.
3. Rickets of prematurity: is seen in some infants on prolonged parenteral hyperalimentation. All infants < 1000 grams birth weight, or those with severe short bowel disease, or on prolonged hyperalimentation, should have a serum Alkaline phosphatase checked at 6 weeks of age (should be < 600 U/Liter) and, if maintained on TPN, every two - four weeks thereafter. The heat labile fractionated portion of alkaline phosphatase is diagnostic for differentiating liver ALP from bone ALP. If the bone fraction is significantly elevated, consider scout bone films
4. Frequently infants with bronchopulmonary dysplasia requiring diuretic therapy will develop a significant hypochloremic metabolic alkalosis. Maximizing the amount of Cl- (or minimizing the amount of HCO3-) provided in the TPN and maximizing the delivery of K+ (watch serum electrolytes very carefully) can help prevent or ameliorate this condition. The usual therapy for this group of infants is supplemental KCl intake.
E. Calcium/Phosphate- due to the risk of precipitation, parenteral administration of Ca/PO4 cannot achieve intrauterine accretion rates (Ca2+ 6-7 mEq/kg/day, PO4 4 mEq/kg/day). Infants on high rates of infusion (200 cc/kg/day) may need lower Ca/PO4 concentrations. Infants requiring high Ca or PO4 will require a decrease in the other component in order to avoid precipitation. It remains somewhat controversial, but most agree that Ca/PO4 should be provided in a 1.5:1 to 2:1 ratio with a goal intake of 3-4.5 mEq/kg/day for calcium and 1.5-2.25 mEq/kg/day of phosphorus. The addition of additional Cysteine to Trophamine helps to lower the pH of hyperalimentation and allow for higher concentrations of Ca and PO4.
F. Iron - infants on long-term parenteral hyperal for over 8-12 weeks may need parenteral iron supplementation in the form of Imferon (iron dextran). Please consult the NICU Pharm D if you are considering starting parenteral iron therapy. Improper use of Imferon can result in acute anaphylaxis reactions.
G. Vitamins
1. Pediatric MVI is currently being used. It is added to parenteral hyperalimentation in the following concentrations (based on patient’s body weight).
a. < 1 kg, 1.5 mL per patient day
b. 1-3 kg, 3.3 mL per patient day
c. > 3 kg, 5 mL per patient day
H. Trace Elements
1. We use the Pediatric Trace Element-5 Solution which is added at a concentration of 0.2 mL/kg/day to the hyperal. Each 0.2 mL contains:
a. Zinc - 200 mcg
b. Copper - 20 mcg
c. Chromium - 0.17 mcg
d. Manganese - 2.5 mcg
e. Selenium - 3 mcg
2. For infants < 2000 grams, we recommend additional Zinc and Levocarnitine
a. Zinc - 200 mcg (for a total of 400 mcg/kg when using PTE-5)
b. Levocarnitine 20 mg/kg/day
3. For infants who have been on hyperal alone for > 4 weeks (28 days), we also recommend adding Molybdenum and Iodine
a. Molybdenum - 0.25 mcg/kg/day
b. Iodine - 1.0 mcg/kg/day
4. Special considerations
a. biliary obstruction - omit copper, manganese
b. renal insufficiency - decrease or omit chromium, selenium
c. catabolic states or ileostomy - add additional Zinc
I. Cysteine addition - we consider cysteine addition critical for two reasons: (1) it enhances Ca/PO4 solubility in TPN and (2) it is a critical component in the synthesis of glutathione, an important anti-oxidant in short supply in neonates. Recommended doses are:
1. < 2 kg: 0.5 mM
2. > 2 kg: 1.0 mM. Infants > 42 weeks generally do not need s supplementation.
Parenteral Hyperalimentation Complications
A. Catheter related accidents
B. Sloughs from infiltrated peripheral IV
C. Sepsis
D. Electrolyte imbalance
E. Hepatic damage
F. Nutritional deficits
G. Central venous thrombosis/obstruction
H. Extravasation of TPN into pleural space
Hyperalimentation lines and solutions must be treated with strict aseptic technique!
I. Who is eligible?
A. Acutely ill infants for whom enteral feedings are not anticipated for 3 or more days.
B. Chronically ill infants for whom you feel the benefits of parenteral nutrition outweigh the risks.
C. Infants with gastrointestinal malformations or injury or severe malabsorption.
D. Most premature infants.
II. When?
A. On admission day if infant is stable and you anticipate a prolonged period of time (i.e., more than 4-5 days) before attaining full enteral feedings. This population would include almost all infants < 34 weeks post menstrual age.
B. Certain post-operative patients - after fluid and electrolyte management is stable.
C. Older infants with acute illness once fluid and electrolyte management are stable.
III. How?
A. Peripheral IV – preferred for short-term access but has limitations
B. Central line (usually PICC line). Central lines are usually placed for long-term intravenous access needs. They can accommodate higher osmolality concentrations of IV fluids (> 1000 mosmoles) versus peripheral IVs.
IV. What?
An order sheet is available in our NICU that outlines orders for glucose, protein and fat administration as well as recommended doses for electrolytes. Ideally, this order sheet must be completed for each patient needing TPN/IL by 14:00 each day. Write TPN/IL orders for infants upon admission if an infant is admitted in the morning so that TPN/IL may be begun that evening.
A. Glucose
1. Amount - up to 20 gm/kg/d (peripheral IVs limited to D12.5 or less). Infants who are fluid restricted to < 120 cc/kg/d may need higher dextrose concentrations (up to D20-25 by Central Line).
2. Method - Start with the solution that provides the gm/kg/d that is being tolerated in previous IVF and increase to maximum over several days. In a first day infant, D10 is usually tolerated well by infants > 1000 grams birth weight. Smaller infants may not tolerate this level of dextrose.
3. Adverse Effects
- hyperglycemia
- glycosuria
- osmotic diuresis
- post-infusion hypoglycemia
4. Monitor
- blood glucose is more accurate than serum glucose
- Fluid input and output (I & O)
B. Protein (as amino acid)
1. Amount - For normal maintenance and growth in most infants, 3-3.5 gm/kg/day of amino acids are adequate - should be 8-15% of total calories. In some rare cases, infants may require more, ( 4.0 gm/kg/day).
2. Method: start with 3.0 gm/kg/d. Increase to 3.5 gm/kg/day the following day, except in the very sickest or smallest neonates (confer with your Attending physician if you have questions). It is important to start protein ASAP in very low birth weight infants as they are highly catabolic without protein supplementation and because concomitant protein administration improves glucose tolerance.
3. Potential Adverse Effects
- azotemia (although recent studies reveal this to be unlikely)
- acidosis (seen when amino acids provide > 15% of total calories)
- serum amino acid imbalance
- hyperammonemia
- ? hepatic injury
- ? cholestasis
- ? neurological injury if > 4.0 gm/kg/day
4. Monitor
- liver function studies (every 7-10 days including GGT, SGOT, SGPT and bilirubin levels )
- ?BUN (see azotemia comments above)
- pH
5. Source - Trophamine is the amino acid formulation available for use in hyperal in the NICU.
Fat - current preparations (soy oil or safflower oil extracts) contain a high content of polyunsaturated fats (double bonds between carbon atoms). Polyunsaturated fats (PUFAs) are essential in the diet (linoleic acid, arachidonic acid, docosahexanoic acid). However, they are also predisposed to rapid decomposition into toxic lipid aldehydes and peroxides via free radical mechanisms. We suggest that for the first several days of life, infants < 750 grams receive limited concentrations of Intralipid supplementation (1 - 2 gms/kg/day of Intralipids). At 3-4 days of life, the < 750 gram infant may then be advanced to 3-3.5 gm/kg/day of Intraplipid. Monitor serum triglyceride levels prior to advancing from 2 gms/kg/day. In addition, because Intralipid components can displace bilirubin from albumin, we recommend that infants with significant risk of kernicterus (i.e., the infant < 750 gms birthweight, the infant with hemolytic anemia, or the asphyxiated infant) be cautiously advanced to maximal Intralipid concentrations.
Maximum amount - 3.0 gm/kg/day. Older, more mature infants who are fluid restricted and experiencing glucose intolerance may require up to 4 gm/kg/day. Fat calories should provide between 40-50% of total calories.
2. Method - begin with 2.0 gm/kg/day. You may advance to a maximum of 3.0 gm/kg/d. Because Intralipids have been associated with an increased risk of nosocomial infections (especially Staphylococcal infections), we recommend infusing them over 18-20 hours rather than over the entire 24 hour day. Beware that some of the smallest and/or sickest infants will not tolerate this shorter infusion intervals.
3. Adverse effects
- displaces bilirubin from albumin (at high doses)
- altered oxygen diffusion secondary to “coating” of the RBC
- altered immune function and associated with increased infections
- altered platelet function
- altered prostaglandin synthesis
- deposited in lungs, liver, spleen (lipid overload syndrome)
- polyunsaturated fats (like Intralipid) are very predisposed to oxidative insult (many investigators think intralipids should be light protected to prevent photo-oxidation)
4. Monitoring
- serum Triglyceride level weekly (should = < 200 mg/dL) or more frequently in very sick or very immature infants
- direct bilirubin weekly
- liver function studies weekly x 1 wk, then q 2 weeks.
5. The lipid dose may need to be decreased to the minimum amount to meet essential fatty acid needs (0.5 gm/kg/day) and the triglyceride level may need to be monitored more frequently in the following conditions:
- hyperbilirubinemia approaching exchange transfusion levels
- liver disease
- sepsis (acute phase)
- severe pulmonary disease
D. Electrolytes (see attached TPN order sheet)
1. These are suggestions only. Some infants will require adjustment more than once/day. Generally those infants requiring very frequent electrolyte adjustments should not be on TPN. However, if this situation is anticipated, TPN may be calculated to provide some % of total fluids and electrolytes and the remainder provided as non-amino acid containing IV fluids which may be changed more frequently and at less expense.
2. When initiating TPN, electrolytes should be monitored q day for 2-3 days and then at least once per week thereafter. Infants receiving the same TPN formulation for long periods of time may need even less monitoring.
3. Rickets of prematurity: is seen in some infants on prolonged parenteral hyperalimentation. All infants < 1000 grams birth weight, or those with severe short bowel disease, or on prolonged hyperalimentation, should have a serum Alkaline phosphatase checked at 6 weeks of age (should be < 600 U/Liter) and, if maintained on TPN, every two - four weeks thereafter. The heat labile fractionated portion of alkaline phosphatase is diagnostic for differentiating liver ALP from bone ALP. If the bone fraction is significantly elevated, consider scout bone films
4. Frequently infants with bronchopulmonary dysplasia requiring diuretic therapy will develop a significant hypochloremic metabolic alkalosis. Maximizing the amount of Cl- (or minimizing the amount of HCO3-) provided in the TPN and maximizing the delivery of K+ (watch serum electrolytes very carefully) can help prevent or ameliorate this condition. The usual therapy for this group of infants is supplemental KCl intake.
E. Calcium/Phosphate- due to the risk of precipitation, parenteral administration of Ca/PO4 cannot achieve intrauterine accretion rates (Ca2+ 6-7 mEq/kg/day, PO4 4 mEq/kg/day). Infants on high rates of infusion (200 cc/kg/day) may need lower Ca/PO4 concentrations. Infants requiring high Ca or PO4 will require a decrease in the other component in order to avoid precipitation. It remains somewhat controversial, but most agree that Ca/PO4 should be provided in a 1.5:1 to 2:1 ratio with a goal intake of 3-4.5 mEq/kg/day for calcium and 1.5-2.25 mEq/kg/day of phosphorus. The addition of additional Cysteine to Trophamine helps to lower the pH of hyperalimentation and allow for higher concentrations of Ca and PO4.
F. Iron - infants on long-term parenteral hyperal for over 8-12 weeks may need parenteral iron supplementation in the form of Imferon (iron dextran). Please consult the NICU Pharm D if you are considering starting parenteral iron therapy. Improper use of Imferon can result in acute anaphylaxis reactions.
G. Vitamins
1. Pediatric MVI is currently being used. It is added to parenteral hyperalimentation in the following concentrations (based on patient’s body weight).
a. < 1 kg, 1.5 mL per patient day
b. 1-3 kg, 3.3 mL per patient day
c. > 3 kg, 5 mL per patient day
H. Trace Elements
1. We use the Pediatric Trace Element-5 Solution which is added at a concentration of 0.2 mL/kg/day to the hyperal. Each 0.2 mL contains:
a. Zinc - 200 mcg
b. Copper - 20 mcg
c. Chromium - 0.17 mcg
d. Manganese - 2.5 mcg
e. Selenium - 3 mcg
2. For infants < 2000 grams, we recommend additional Zinc and Levocarnitine
a. Zinc - 200 mcg (for a total of 400 mcg/kg when using PTE-5)
b. Levocarnitine 20 mg/kg/day
3. For infants who have been on hyperal alone for > 4 weeks (28 days), we also recommend adding Molybdenum and Iodine
a. Molybdenum - 0.25 mcg/kg/day
b. Iodine - 1.0 mcg/kg/day
4. Special considerations
a. biliary obstruction - omit copper, manganese
b. renal insufficiency - decrease or omit chromium, selenium
c. catabolic states or ileostomy - add additional Zinc
I. Cysteine addition - we consider cysteine addition critical for two reasons: (1) it enhances Ca/PO4 solubility in TPN and (2) it is a critical component in the synthesis of glutathione, an important anti-oxidant in short supply in neonates. Recommended doses are:
1. < 2 kg: 0.5 mM
2. > 2 kg: 1.0 mM. Infants > 42 weeks generally do not need s supplementation.
Parenteral Hyperalimentation Complications
A. Catheter related accidents
B. Sloughs from infiltrated peripheral IV
C. Sepsis
D. Electrolyte imbalance
E. Hepatic damage
F. Nutritional deficits
G. Central venous thrombosis/obstruction
H. Extravasation of TPN into pleural space
Hyperalimentation lines and solutions must be treated with strict aseptic technique!