FLUID AND ELECTROLYTES
I. Principles
A. Calculate fluid and electrolyte maintenance on a per kilogram basis.
Most stock intravenous solutions are generally not tailored for
the special needs of preterm babies.
B. Estimate fluid and electrolyte losses.
C. Monitor adequacy of therapy.
D. Fluid balance is a dynamic process for newborn.
II. Normal maintenance
A. Na+ = 0 -3 mEq/kg/day (NS = 154 mEq/L; 1/2 NS = 77 mEq/L; 1/4 NS = 38 mEq/L). Small preterm infants during the first several days of life may need no additional sodium at all. After the first weeks of life they may require more sodium, especially if urinary losses increase secondary to drug use side effects).
B. K+ = 0 - 2 mEq/kg/day - do not add to fluids of very small infants (< 700-800 gms birth weight) until they have demonstrated a need for K+.
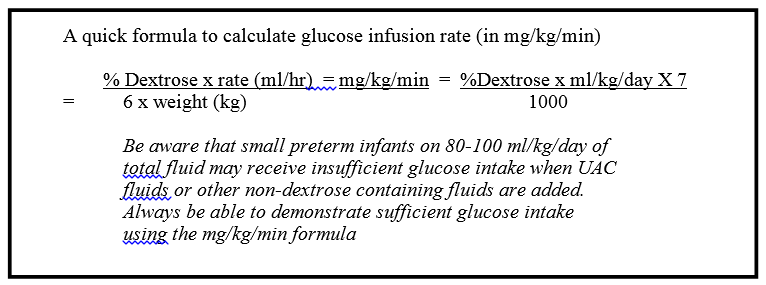
C. Glucose: start with D10W and observe closely for glycosuria. The normal maintenance requirement of glucose is 5-8 mg/kg/minute. Extremely low birthweight babies < 750 gm may need to be started on D5W.
D. Fluid for a normal term (> 2500 gms birthweight) newborn:
1. 1st 24 hours: 80-100 ml/kg/day with no electrolytes
2. 2nd day: 100-120 ml/kg/day with electrolytes
3. 3rd day: 120 ml/kg/day with electrolytes
4. 4th day: 140 ml/kg/day with electrolytes
E. Fluid for a normal preterm newborn:
1. < 750 gms = 60-90 ml/kg/day (1st day of life) These infants should be in incubators with humidity (70%-80%) beginning on DOL #1
3. 1001 - 1500 gms = 80-100 ml/kg/day (1st day of life)
4. 1501 - 2500 gms = 90-100 ml/kg/day (1st day of life)
All ELBW infants (< 1000 grams birth weight) should be in humidified incubators on DOL #1. The incubators should be maintained at 70%-80% humidity for the first 7 days of life at which time the skin should begin to be sufficiently keratinized to prevent excessive free water losses. For these smallest of babies, very immature skin may result in extreme free water losses resulting in free water requirements in excess of 150 ml/kg/day.
III. Normal Losses
A. Insensible water loss = 35-40 ml/kg/day (may increase under radiant warmer or phototherapy, or in the very small preterm infant).
B. Urine output should be > 1-2 ml/kg/hour.
C. Maximum expected weight loss in the first few days of life is 10-15% of birthweight (may be delayed in babies with respiratory diseases who are receiving additional free water through the isothermic and humidified portion of the ventilatory circuit).
IV. Monitoring Fluid and Electrolytes in Critically Ill Babies.
A. Daily weights, daily input (ml/kg/day) and output (urine + GI + stool, etc.), are important variables to follow. Useful laboratory parameters to follow include serum electrolytes, BUN, creatinine and glucose and occasionally urine electrolytes and specific gravity. In infants with BW < 1.0 kg, we generally prefer minimal stimulation (thus, patients are not weighed unless specifically requested or weight is recorded by an electronic bed scale that may not always be accurate). However, in some cases of severe weight losing disease, we may need to monitor weight BID and serum electrolytes more often than just daily.
B. Monitor intravascular status. A CVP may be clinically helpful.
C. Fractional excretion of sodium
1. Urine Na/Serum Na x 100 = Fract Exc. of Na.
Urine Cr/SerumCr
2. > 2.5% consistent with renal failure
3. Only useful as renal failure index if patient is oligouric
4. Usually unreliable in preterm infants
5. Unreliable after Lasix.
V. Special Situations
A. Hyponatremia – or low serum sodium values – may be caused by either excessive sodium losses over time or by fluid retention with resulting dilutional hyponatremia. Of these two etiologies, by far the most common etiology for hyponatremia during the first week of life is Dilutional Hyponatremia. In order to correct dilutional hyponatremia, it is usually necessary to restrict both fluid AND sodium administration. It is usually incorrect to assume that low serum sodium means “needs more salt” – most often it is the opposite – “needs salt restriction.” For example, if an infant has received numerous volume expansions with normal saline and has had decreased urine output, then certainly the diagnosis is dilutional hyponatremia. Be aware that after the first week of life hyponatremia may increasingly be associated as an indirect marker of sepsis (especially in the very low birth weight infant).
Diuretic therapy works by causing increased salt excretion into the urine, thereby increasing salt and fluid elimination. If one needs to get rid of salt and fluid, you should prescribe a diuretic. Therefore, it is almost always incorrect to administer salt AND give diuretic therapy.
B. Post-asphyxia - observe for complications of multi-organ dysfunction including acute tubular necrosis (ATN), cerebral edema, and tricuspid insufficiency.
1. initially restrict fluids to insensible loss plus urine output with no added Na+ or K+. It may be helpful to write the fluid order with ml/ml UOP replacement up to a maximum of what expected fluid needs would be.
2. if the infant urinates and urinalysis is normal, may increase fluid appropriately.
3. if post-ischemic ATN is present, urinalysis will reveal protein and RBCs; BUN and creatinine will rise, urine output initially will be decreased and demonstrate an increased urine Na+ loss (% F.E. of Na > 2.5).
4. when an infant recovers from ATN, he or she may have a post-ATN diuresis.
C. PDA - premature infants may have an increased risk of developing symptomatic PDA with excessive fluids.
1. Although excessive fluids may exacerbate a PDA, dehydrating an infant will not cause it to close.
2. Indomethacin is the most acceptable form of therapy for a symptomatic PDA. However, it can produce significant renal complications ranging from transient oliguria to renal failure (dose dependent). Before ordering indomethacin, make sure infant is adequately hydrated, UOP > 1 ml/kg/hr and Cr < 1.5. If renal status is questionable, the overall risk/benefit of administering the drug must be discussed.
D. Post-gastrointestinal surgery
1. Observe for third space loss of fluid
2. A post-operative infant’s fluid requirements depend on the underlying pathology and operative procedure performed. (Peritonitis needs large amounts of fluids, diaphragmatic hernia babies need 2/3 - 3/4 of maintenance).
3. Replacement of gastrointestinal losses (from suction) required when volume is significant ~ 10 ml/kg/shift. May start replacement with 1/2 NS + 20 mEq KCl/Liter @ ml/ml every 4 hours. Sending a gastric fluid sample to the lab can help determine exactly what electrolyte composition is needed for replacement in those infants with very large gastric fluid losses.
E. Intensive Care Infants
1. Infants with respiratory disease generally have a delay in normal weight loss beyond the first few days.
2. Fluid needs should be calculated on basis of weight changes, urine output, BUN, etc. rather than simply picking ml/kg based on age.
3. Edematous infants (e.g. some hydrops infants, some post-op infants) may still be intravascularly depleted.
4. Medications:
- most are given as a slow push in 5-10 minutes
- for fluid calculation, assume 1.5 ml per flush per medication
- Potassium boluses can be very dangerous. The need for a potassium bolus should always be discussed. The dose is 1 mEq/kg given over a minimum of 2 - 6 hours.
- Calcium should be given over 60 minutes (most frequently given as calcium gluconate. The gluconate moiety requires good liver function for conversion to ionic form. Non-emergent NaHCO3 can be given over 20-30 minutes in the term infant and 60 minutes for the preterm infants. Dilute 1:1 with water.
- Aminoglycosides, Vancomycin, and Aminophylline are generally given over 30-60 min.
- Intralipid is counted in total fluid calculation
- Calcium and NaHCO3 cannot be mixed with each other or anything else.
5. Arterial lines
- run 1/4NS to NS with 0.5-1.0 units heparin/ml for peripheral arterial lines (PAL longevity may be increased with Papaverine, 6 mg in 50mL).
- UACs are less prone to clot if run with the above fluids. For small babies, normal saline may result in excessive sodium. D5W, 1/8 NS or 1/4 NS with heparin may be more appropriate for the first several days of life for these more premature infants. Flush fluid may also need to be sodium restricted in very small infants (use 1/4 NS).
- Don’t forget arterial line sodium when calculating total daily sodium for an infant (especially the extra low birthweight infant).
F. Skin care, Humidified Incubators and the ELBW infant (< 1000 grams)
Whenever possible, these infants should be transferred to a humidified incubator within the first 24-48 hours of life. Typically, the humidity should be set at 70% - 80% and the infant should remain in this environment for the first 7 days of life. After this time, the humidity is lowered to 50% for 7 days (at which time the skin is more fully keratinized). In addition, this group of infants should have skin care optimized to prevent excessive fluid losses.
VI. Fluid Types
Remember: Replace intra-vascular losses with colloid
Replace fluid losses with water or crystalloids
Replace electrolyte losses with electrolytes
