Hypoxic Ischemic Encphalopathy
Perinatal asphyxia, more appropriately known as hypoxic-ischemic encephalopathy (HIE), is characterized by clinical and laboratory evidence of acute or subacute brain injury due to asphyxia.
|
|
|
Diagnosis
*Hypothermia for moderate to severe encephalopathy
Requirements:
Requirements:
- History of acute perinatal event (placental abruption, cord prolapse, severe fetal distress)
- An Apgar score <5 at 10 minutes
- Cord pH or any postnatal blood gas pH at < 1 hour < 7.0.
- Base deficit on cord gas or any postnatal blood gas at < 1 hour > 16 mEq/L.
- Continued need for ventilation initiated at birth and continued for at least 10 minutes.
|
IF BLOOD GAS AVAILABLE INFANT SHOULD HAVE 3 OR 4 FROM ABOVE LIST.
|
IF BLOOD GAS IS NOT AVAILABE, OR pH 7.01 TO 7.15, OR BASE DEFICIT 10 TO 15.9 mEq/L INFANT SHOULD HAVE 1 AND 2 OR 5 FROM ABOVE.
|
Once infant meets either of the above criteria, proceed to neurologic examination.
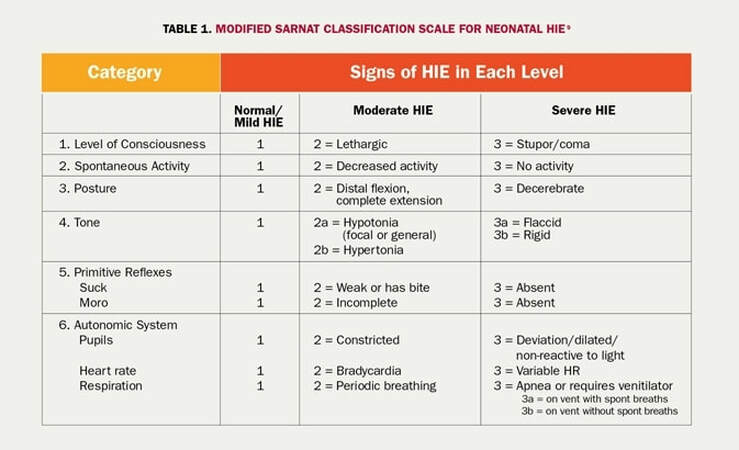
The presence of moderate/severe encephalopathy defined as seizures OR presence of one or more signs in 3 of the 6 categories (level of consciousness, spontaneous activity, posture, tone, primitive reflexes and autonomic system).
Treatment
Supportive Care
Physiologic Effects of Hypothermia
- Maintain O2 and CO2 in normal ranges
- Monitor and maintain normal arterial blood pressure
- Administer volume slowly; overall fluid restriction
- Monitor electrolytes and glucose
- Control seizure activity
- Lower core body temperature (current protocol lowers patient's core temp to 33.5 Celcius for 72 hours then rewarm slowly over the next 8 -12 hours)
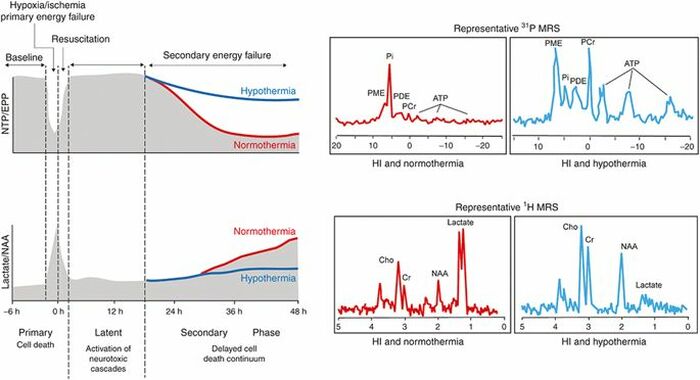
Physiologic Effects of Hypothermia
- Inhibition of excitatory oxidative cascade (decreased glutamate, lactic acid and iNO)
- Inhibition of mitochondrial failure
- Inhibition of free radical damage
- Inhibition of proteases and caspase
- Anti-inflammatory
- Inhibition of lipid peroxidation
- Reduction in apoptosis
Alistair, J. Pediatric Research volume 81, pages 202–209 (2017)
Prognosis
Therapeutic hypothermia reduces death and disability among infants with neonatal encephalopathy. In a systematic review of 1214 neonates with hypoxic-ischemic encephalopathy (HIE) who were treated with therapeutic hypothermia, nearly one-half either died or had major neurodevelopmental disability at 18 months, while 40 percent had a normal neurologic outcome.
MRI is obtained at 4-7 days of life following rewarming to aide in diagnosis. Normal MRI obtained following therapeutic hypothermia is associated with normal neurologic outcomes. Abnormal MRI findings are associated with worse neurologic outcomes, however there is limited evidence of direct correlation with MRI findings and neurologic outcome.
MRI is obtained at 4-7 days of life following rewarming to aide in diagnosis. Normal MRI obtained following therapeutic hypothermia is associated with normal neurologic outcomes. Abnormal MRI findings are associated with worse neurologic outcomes, however there is limited evidence of direct correlation with MRI findings and neurologic outcome.
