ENTERAL FEEDING
I. Selection of Formula - determining factors
A. Availability of breast milk (THE PREFERRED ENTERAL FEEDING OF CHOICE)
B. Size and gestational age
1. Newborn infants less than 1800 grams need IVF to prevent hypoglycemia as it will require several days to advance them to full enteral feedings.
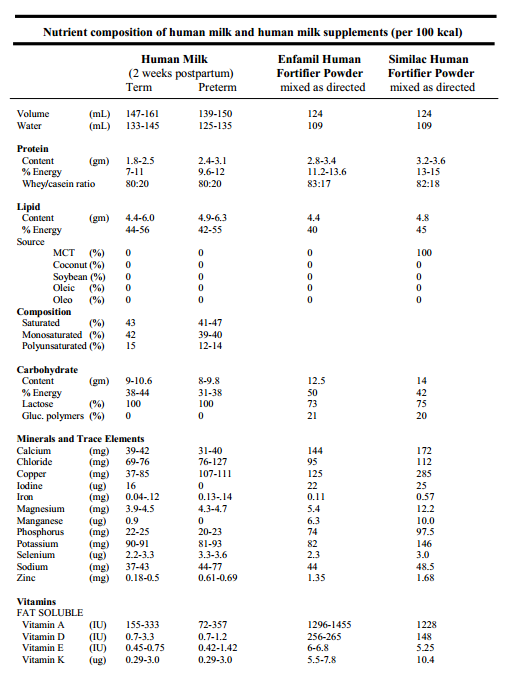
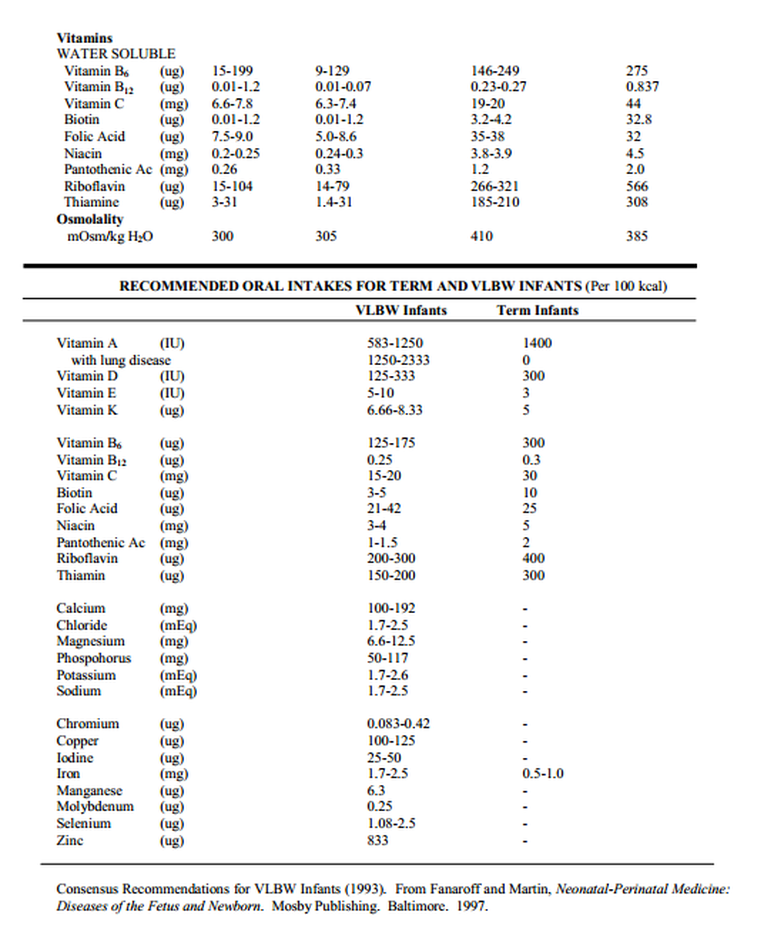
2. Preterm infants require increased caloric density, increased Na+ content, more protein, and more Iron, Calcium and Phosphate than term infants.
3. All formula fed infants should be started on an iron-containing formula with the initiation of feedings.
C. Associated Pathology
1. Impaired renal function or heart disease with congestive heart failure - these infants need lower Na+ content.
2. Post-operative removal of small intestine - elemental formulas for improved absorption may be required.
D. See table at end of chapter for detailed list of formula content.
II. Section of Method of Feeding
A. Determining Factors
1. Size and Gestational Age
a. infants less than 32-34 weeks post menstrual age lack the neuromaturation to have a coordinated suck and swallow and an effective gag reflex. This makes oral (po) feeding dangerous. Once you decide to try po feeding, determine post-menstrual age, check for an effective suck and swallow and gag reflex and use sterile water for the first attempt.
b. infants < 32-34 weeks need to be fed NG or OG and then continue to be supplemented this way until taking adequate volume and calories by mouth.
c. healthy term infants should be kept NPO x 4 hrs and then fed po ad lib after 10 cc of sterile water or breast milk (aspiration of breast milk is no worse than sterile water). Term infants can then be fed on demand after this first feed.
2. Associated Pathology
a. acutely ill infants should only receive trophic feeds (if any at all!) when using an enteral route.
b. respiratory illness: generally do not attempt po feeds in an infant for whom feedings would otherwise be appropriate until the RR is < 60 breaths per minute (there may be legitimate exceptions). Also, formula in the GI tract will increase O2 consumption. Therefore, in general, infants with respiratory distress are kept NPO until they are in < 40% FIO2 and have RR < 60-70. Some BPD infants and some other infants (persistent TTN) may be considered exceptions to this rule.
c. GI pathology - if surgical repair of congenital obstruction, atresia or perforation has been required, the decision of when and how to initiate feeds needs to be made in conjunction with the Pediatric Surgical Service. In general, resolution of post-op ileus (cessation of bilious upper GI output) and ability to handle secretions is the very minimum criteria to be met before feeds can be started.
d. Reflux - gastric reflux exists in almost every premature infant secondary to decreased esophageal motility and a dysfunctional lower esophageal sphincter. Significant reflux may contribute to feeding intolerance, induction of hypervagal (apnea and bradycardia) responses and potential for microaspiration. Feeding regimens for the group of infants with significant reflux are highly variable and depend on results of esophageal pH/manometry studies and contrast studies of swallowing and gastric outlet anatomy. Continuous feeds, thickened feeds, positioning, and medications to decrease acidity and improve GI motility may be required separately or in combination.
B. Methods
1. OG/NG - most commonly used
a. estimate appropriate distance and check for proper tube placement by auscultation over stomach or confirm placement with X-ray
b. NG tubes do cause partial airway obstruction. Consider making NPO or changing to an OG tube if an infant has significant apnea.
c. OG tubes are more easily displaced into esophagus or pulled out.
d. presence of tube may induce GER by stenting open lower esophageal sphincter.
e. caffeine may exacerbate GER
f. when feeding, allow formula to run in by gravity.
2. Transpyloric - rarely used, only continuous feeding is allowed.
a. indication: infants who have failed gastric feedings.
b. have same disadvantages of OG/NG tubes plus lack of normal intermittent feeding pattern. An increased risk of NEC has been reported.
c. check position with X-ray. Normal duodenal/jejunal aspirate pH should be 5-7.
C. Advancing Feeds
In general, healthy term infants take 4-5 days to reach full feeds when mothers choose to breast feed. Empirically and statistically, sick and preterm infants do better when advanced more slowly (10 - 14 days to full feeds).
D. PROTOCOL FOR ENTERAL FEEDS IN THE PRETERM INFANT
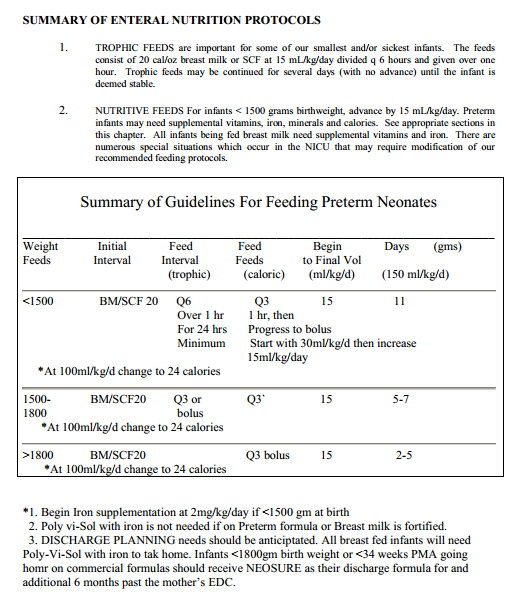
NON-NUTRITIVE FEEDS aka TROPHIC FEEDING : there is now evidence in the literature supporting the fact that small, non-nutritive, enteral feedings can benefit the preterm infant by inducing secretion of endogenous gastrointestinal motility agents and digestive enzymes and by enhancing intestinal mucosal maturation. Institution of small, non-nutritive, enteral feeding (or trophic feeds) has resulted in better feeding tolerance, improved absorption patterns and shorter hospital stays.
In general, trophic feeds are reserved for the smallest and most at-risk infants ( less than 1500g). However, other infants may be fed trophic feeds based on the clinical scenario and attending discretion. Trophic feeds generally will be instituted before advancement to nutritive feeding schedules. In our NICU trophic feeds are initiated by giving 15ml/kg/day divided q 6 hours. The feeds will be given over one hour.
NUTRITIVE FEEDING SCHEDULES Based on the current feeding recommendations of several sources, it has been demonstrated that improved feeding tolerance, better weight gain and less necrotizing enterocolitis (see Chapter 19) are seen when preterm infants are advanced to full enteral feeds slowly. In our NICU, nutritive feeds are initiated by giving the trophic feeding volume every three hours rather than every six hours (an increase of 15 ml/kg/day). These feeds are given over one hour. An increase of 15 mL/kg/day is continued until the baby is on 150 mL/kg/day. When a baby reaches 100 mL/kg/day, then will be changed to 24 cal/oz breast milk or formula.
E. Calories: term infants need at least 100 kcal/kg/day to maintain body weight and but generally require 110-120 kcal/kg/day to gain weight. Preterm infants may need more (110-140 kcal/kg/day). Proprietary formulas for term infants and breast milk from term infant mothers have caloric densities of 20 kcal/oz (thus, term infants need 150-180 cc/kg/day for proper growth). Preterm formulas have caloric densities of 24 kcal/oz (thus, preterm infants need 135-175 cc/kg/day for proper growth). Breast milk for preterm infants should be supplemented (there are a variety of ways to do this) to provide 24 kcal/oz as preterm infants often times will not tolerate volumes of enteral feeds equivalent to or greater than 180 cc/kg/day.
F. Residuals: it has been common practice in the NICU to follow gastric residuals in all premature babies. In our NICU residuals are not checked unless there is evidence of intolerance such as abdominal distention or emesis. If checked and < 50 % of a feeding, the nursing staff will refeed the residual and subtract it from the next feeding continuing the advance. If it is > 50% of the feed, it will be refed, subtracted from the next feed, and the advance will be held until < 50%. If residuals greater than 50% are found with 2 feedings in row, then the house officer will be notified.
III. Monitoring Feeds
A. Appropriate feeding should allow weight gain of 20-30 grams/kg/day
B. In addition, tolerance can be gauged by:
1. Physical exam – normal bowel sounds, lack of abdominal distension, etc.
2. Stooling pattern (breast milk fed infants stool more than formula fed infants).
3. Emesis - bilious emesis should be considered evidence for obstruction until proven otherwise.
4. NG aspirates - small volumes (< 10% of feeding) in an otherwise normal infant are generally acceptable, large volumes have been associated with the possibility of more serious illness.
5. Presence of blood in stool - causes range from anal fissure to necrotizing enterocolitis. Positive guaiac tests frequently occur in normal babies with NG tubes in place. Examine the stool and the infant carefully - do not automatically place NPO.
IV. Breast Feeding - in general should always be encouraged!
A. Storage for gavage feeding of preterm infants
- our NICU does not use pooled breast milk at this time
- mothers who wish to breast feed are taught to express breast milk into sterile containers which can then be frozen for up to a month for use for their baby.
- mothers should continue to be encouraged to express breast milk for their child; an oftentimes difficult task for the mother of a micropremie who may be hospitalized for 3 - 4 months.
B. Composition of Breast Milk
- initially, milk from mothers who have had preterm infants differs in having more fat and protein, more sodium and calcium, and more zinc. This difference in content will only last for 3/4 - 1.5 months, after which time, the fat, sodium, and calcium and phosphate content decrease.
- because preterm infants may require additional sodium, calories, calcium, phosphorus and vitamins, the addition of Enfamil or Similac Human Milk Fortifier to the milk will meet all of these needs (with the exception of no (EHMF) or limited (SHMF) fat calories). Use of microlipids (medium chain triglycerides) can help supplement potential fat deficiencies. For Moms with an insufficient breast milk supply, the addition of Similac Natural Care should be considered. Mixing BM with Natural Care in a 50:50 ratio provides a caloric density of 22 kcal/oz. If Natural Care supplementation has a fault, it may be because it decreases the whey protein content of BM (which is where all of the protective immunoglobulins and maternal enzymes associated with digestion are found) and because some infants will need additional calories in excess of 22 kcal/oz.
V. Vitamin and Mineral Supplementation
A. Vitamin D Supplementation for Preterm Infants
1. Once a preterm infant (< 1500 grams at birth) is switched to a proprietary TERM formula, he will not receive adequate Vit D until he is consuming one liter/day of formula. Once on Similac, Enfamil, etc. order 0.5 cc/day of a Pediatric Multivitamin. This will need to be continued after discharge and ordered as a discharge prescription (for the preterm infant only).
2. All breast fed babies need to receive vitamin D and iron supplementation which should be continued after discharge. Use 0.5 cc/day of a Pediatric Multivitamin preparation with Fe (such as Poly-Vi-Sol with Fe).
B. Iron
1. All infants should be started on iron-containing formula with the initiation of feeds.
2. Iron use is especially important in premature infants, particularly in helping to prevent anemia of prematurity. Iron absorption is to some extent dependent on concomitant administration of Vitamin C. Both are contained in adequate quantities in proprietary premature formulas with iron. Nevertheless, many experts have recently recommended additional supplementation of iron for the preterm infant:
< 1500 grams 2 mg/kg supplemental elemental Fe
In order to simplify Fe administration, it is currently recommended that our NICU infants receive the following iron and vitamin supplementations when near full feeds:
1. All infants < 1500 grams at birth should receive Fer-In-Sol (5 mg elemental Fe per 0.5 mL).
2. Any infant being fed unfortified breast milk should be placed on PVS with Fe, 0.5 mL/day (including after discharge to home)
REFERENCES:
1. Nutritional Needs of the Preterm Infant: Reginald Tsang (ed). Williams and Wilkins Publishers, Baltimore, 1993.
2. Primary Care of the Newborn; Johns Hopkins Center. Mosby Yearbook Publishers, 1993.
3. “Enteral Nutrition of the Preterm Infant”. Steven Gross and Terry Weigle in Clinics in Perinatology. March 1995.
VI. Special Feeding Situations
A. SGA infants: these infants may need additional calories for “catch-up growth.” If one wants to provide additional calories, calculate fluid and calorie requirements on a reasonable weight (10%) for their gestational age and aim for this if this volume is not an extraordinary amount (e.g., > 200 cc/kg/day, 130 - 160 kcal/kg/day). May need a more calorically dense formula (e.g. 24-30 kcal)
B. Asphyxiated babies: probably should not be fed -- or be fed very cautiously -- for 3 - 5 days, certainly don’t feed them if they have an ileus. Infants who are at high risk of asphyxial injury are those with cord pH < 7.00, infants with Apgar scores < 3 at 5 minutes of age, those infants requiring CPR early in life, infants with significant CNS abnormalities and those infants with significant cardiorespiratory support requirements
C. IDM: these infants need to be fed early and may also require additional IV fluids to prevent hypoglycemia. Additionally, they may be poor and/or slow feeders.
D. Infants with cholestasis should NOT be fed Portagen as the essential fatty acid content is marginal at 3% of calories (EFAs are critical to normal brain and retinal development). These babies have inherent fat absorption problems that may put them at risk for EFA deficiency on Portagen. Both of the elemental formulas Pregestimil and Alimentum may be more appropriate.
E. BPD Infants: infants with BPD oftentimes need additional calories to grow new lung (a high proportion of their metabolic expenditure is spent breathing). They also need appropriate distribution of their calories (the greater the fat content vs. the carbohydrate content, the less likely you are to produce CO2 - the R/Q ratio - thus, decreasing the amount of respiratory effort spent eliminating PCO2. Finally, these infants need reduced free water intake (to decrease pulmonary edema); thus, these babies may be on 30-32 kcal/oz formula, supplemented with a lot of fat, and on 100-130 cc/kg/day of restricted fluid intake.
F. Preterm Infant Going Home on Commercial Formula: because preterm infants may continue to require additional protein and minerals, it is currently recommended that infants < 1800 grams birthweight or < 34 weeks PMA who are feeding commercial preterm formulas be discharged to home on NEOSURE (or other approved premature/transitional infant formulas). Current recommendations are to use NEOSURE until the infant is at least 4-6 months past the estimated due date of the mother. Because this policy has now been in place for 7 years, we have now begun to appreciate a significant increase in parental complaints about NEOSURE. It is expensive, hard to locate in grocery stores, and appears to cause constipation in some infants. Alternative sources of supplemented commercial formulas may need to be considered in some infants who would be candidates to receive NEOSURE at discharge.