NEONATAL SEPSIS
I. Incidence
1/500 - 1/1600 live births with early onset sepsis
Early onset sepsis is 3 - 10 fold more likely in premature infants
Males have a higher incidence of early onset sepsis than Females
II. Etiology
A. Host Factors
1. Decreased chemotaxis
2. Decreased phagocytosis
3. Decreased bactericidal activity
4. Abnormal metabolic reserves
5. Decreased complement
6. IgG level is maternal/placental dependent - majority crosses placenta in 3rd trimester. Specific antibody may be absent in mother’s pool of antibody
7. Low neonatal IgM and IgA levels.
B. Perinatal Factors
1. Ascending infection
2. Prolonged rupture of membranes
3. Instrumentation / manipulation
4. Internal fetal monitoring
5. Indwelling foreign bodies - UAC, UVC, percutaneous lines, ETTs, IVs
6. Skin breakdown
7. Nosocomial
III. Signs and Symptoms – are extremely non-specific. Suspected sepsis may be associated with (but not limited to) the following:
A. Respiratory distress - may mimic RDS, TTN, etc.
B. Shock and poor perfusion
C. Metabolic acidosis or electrolyte abnormalities (hyponatremia, hyperkalemia)
D. Temperature instability - increased or decreased
E. Abdominal distension, vomiting, ileus
F. Lethargy, irritability
G. Seizures
H. Petechiae, purpura, oozing, other signs of DIC
I. Hypo or hyperglycemia - particularly if a previously stable glucose requirement.
J. Jaundice - particularly an elevated direct bilirubin fraction
IV. Laboratory Diagnosis
A. Blood Cultures - (minimum 1 cc per culture bottle) including cultures from the UAC, central lines, etc. If cultures are being obtained from a central line, also obtain a sample peripherally. If you request a quantitative blood culture on a paired set, you can use the information to determine if a central or arterial line needs to be removed. A high colony count from a central line and a lower count peripherally indicate that you should strongly consider line removal.
B. CSF - LPs should not be performed in unstable patients (e.g. those with DIC, severe respiratory distress, severe apnea, etc.) An LP is not part of the routine sepsis evaluation in an infant immediately following birth. However, an LP should be considered part of the sepsis evaluation in admitted infants with maternal exposure to antibiotics, positive blood cultures in the newborn period and/or with CNS symptoms.
Lumbar punctures in late onset sepsis (“nosocomial”) evaluations
In ALL infants older than 7 days who present with signs of sepsis, an LP should be performed at the time of the sepsis evaluation .
Remember that it is possible to acquire nosocomial neonatal meningitis without bacteremia!
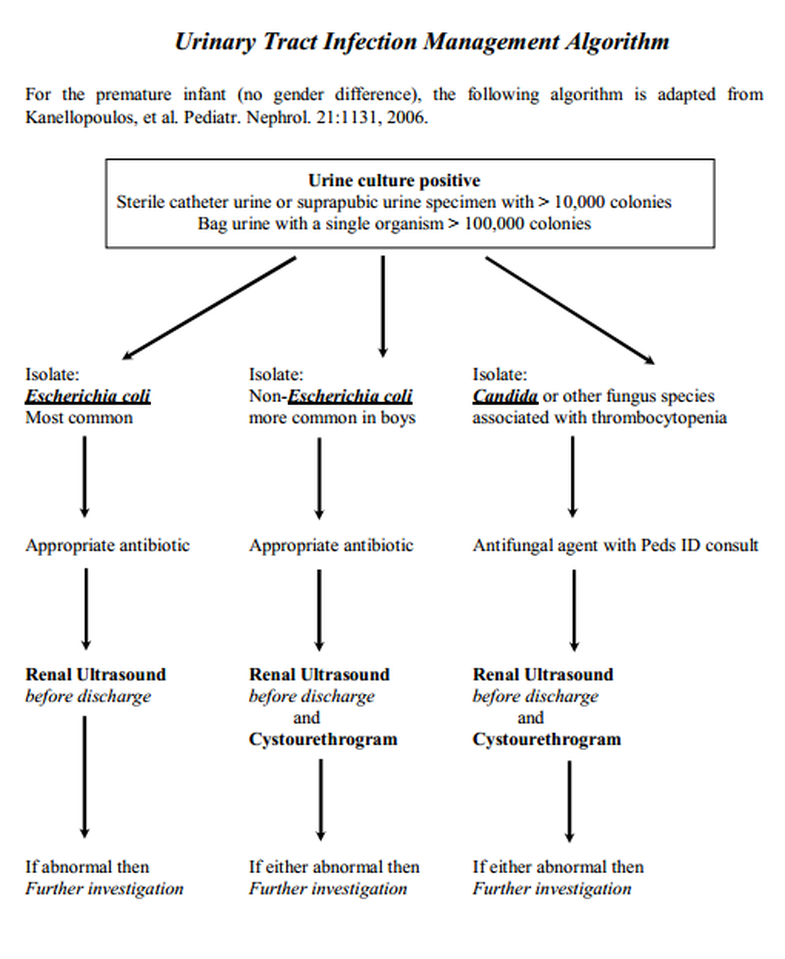
C. Urine - important especially after the first 48 hours of life. Infants are not born with UTIs; therefore, urine cultures are not indicated in a sepsis evaluation immediately after birth (please see comments at the end of this chapter on UTIs in infants).
D. Surface Cultures (axillary, nasopharyngeal, rectal) are NOT indicated except in infants > 24 hours old or transferred from other hospitals or admitted from home.
E. White Blood Cell count - total neutrophil and band count. Sepsis more likely if:
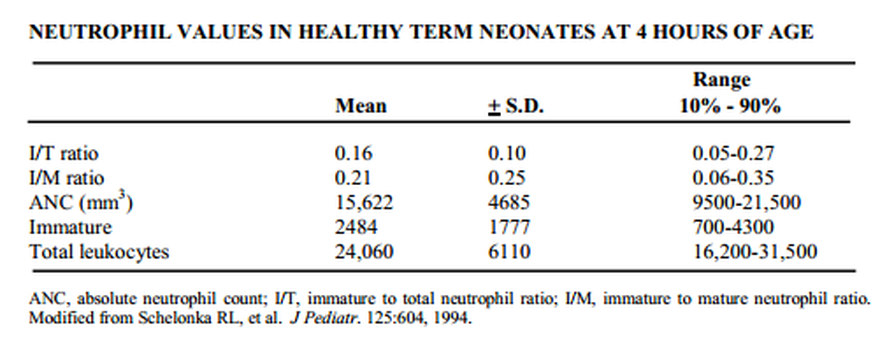
1. Marked shift to the left is present, i.e., immature/total count > 0.2 - 0.25.
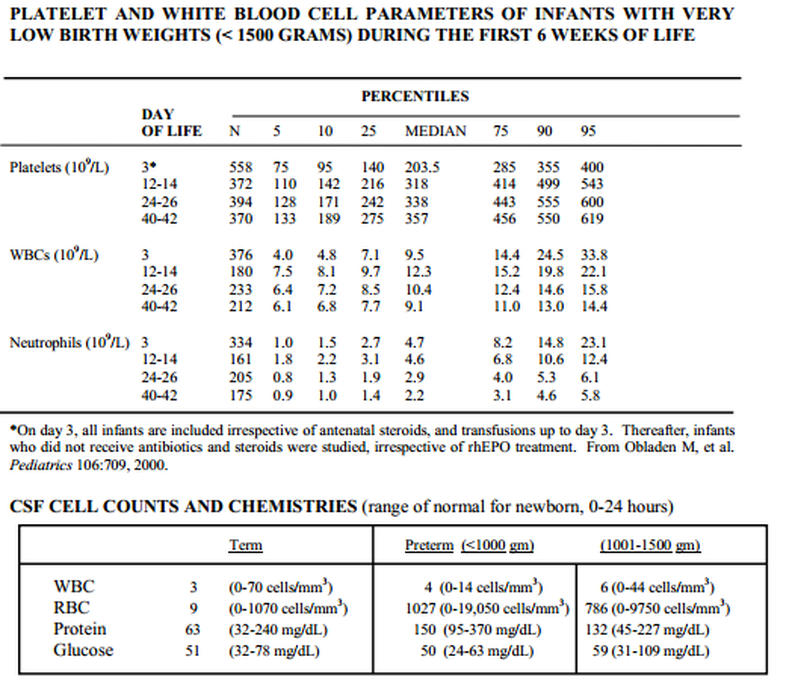
2. Neutropenia - value dependent on age (see chart)
3. Leukocytosis - see chart
F. Other tests: C-reactive protein testing (CRPs) may prove helpful. This test appears to have greatest reliability in late onset sepsis and in following trends after initiation of appropriate therapy. CRP tests are less useful in brand new newborns (but CRP cannot cross placenta from Mom) and in late onset Staph. epidermis infections. They are not likely to be helpful initially in predicting sepsis (positive predictive value) or in helping to determine the need for a sepsis evaluation and antibiotic therapy. The CRP is more useful in predicting the absence of sepsis or other inflammation (negative predictive value).
V. Treatment (Early treatment is essential)
A. Antibiotics: first line is Ampicillin and Gentamicin in the first 7 days of life; Vancomycin and Gentamicin in older infants, especially if a central line is present. During periods of outbreaks of unusual or resistant organisms, these antibiotic choices may change. Monitor levels when appropriate. Adjust antibiotic regimen when organism and sensitivities are identified.
B. Volume expansion/pressors as necessary
C. Monitor:
1. fluid-electrolyte status
2. acid-base status, blood gases
3. Hematocrit, WBC, platelets for evidence of bleeding/DIC.
VI. Nosocomial Infections (serious infections acquired after 3 days of age)
The incidence of nosocomial infection is most common in the very premature infant. There is a 50% incidence in infants < 750 grams birthweight and 15% in infants > 1500 grams birthweight. The most common organisms are Staphylococci (S. epidermis = 40%) followed by gram-negative organisms (25%) and fungi (10%). The risk of death ranges from 5-10% for S. epidermis infections to 40-50% for gram-negative organisms and fungi.
Factors associated with nosocomial infections in NICU patients that are somewhat under the control of the medical staff include indwelling catheter duration, number of days on the ventilator, number of days on total peripheral hyperalimentation, and number of previous infections. Controlling for all epidemiological and management factors, the average length of stay of NICU infants who acquire a nosocomial infection is increased by 28 days which equals approximately $60,000 of hospital costs!
Thus, the index of suspicion should be high for nosocomial infection particularly for the very small infant. In addition, infants who could have central or PICC lines removed or who could come off the ventilator, should have this done. Finally, antibiotics should be used prudently and judiciously. Vancomycin-resistent enterococci have been reported in our hospital and Vancomycin-resistent Staphylococci have been reported in the U.S. and other countries.
In order to reduce the incidence of nosocomial infections in the NICU, it is critical to emphasize the importance of HANDWASHING before and after any patient contact. In addition, it is critically important to maintain a clean environment (including all equipment) around the baby. These infants are more susceptible to infection than any adult chemotherapy patient.
Please be diligent about following good handwashing and clean environment regulations and don’t hesitate to let others know how important this is!!!