HYPERBILIRUBINEMIA
I. Conjugated versus unconjugated (direct versus indirect) bilirubin
The differential diagnosis and the implications of direct vs. indirect hyperbilirubinemia are very different. Free, unbound, unconjugated bilirubin can cross the blood brain barrier and is neurotoxic. It is the more common neonatal problem. Direct hyperbilirubinemia is much less common, not neurotoxic, but is often associated with serious medical/surgical problems. The following material is aimed primarily at the problem of indirect hyperbilirubinemia.
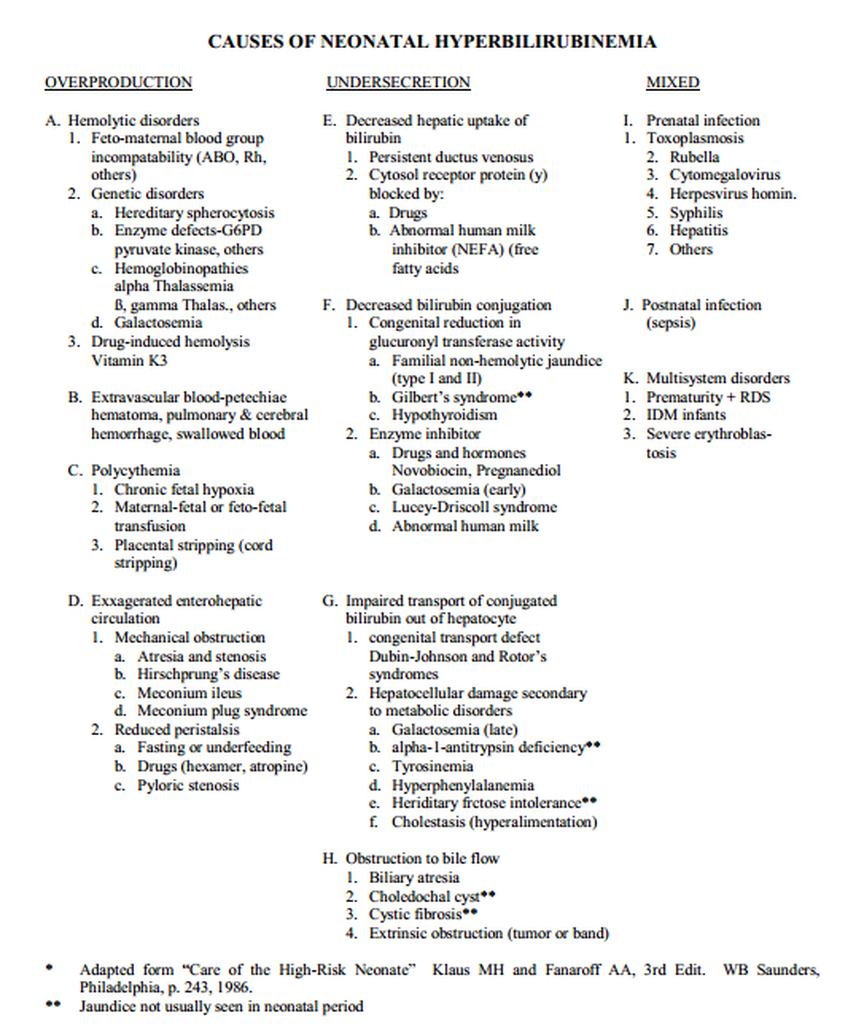
II. Causes of Indirect Hyperbilirubinemia
A. Physiologic jaundice - most neonates develop a mild elevation of bilirubin which represents the effects of a variety of physiologic factors in the newborn (increased red blood cell turnover, decreased Y and Z ligand transport of indirect bilirubin into the hepatocyte and decreased hepatic glucuronidase conjugation):
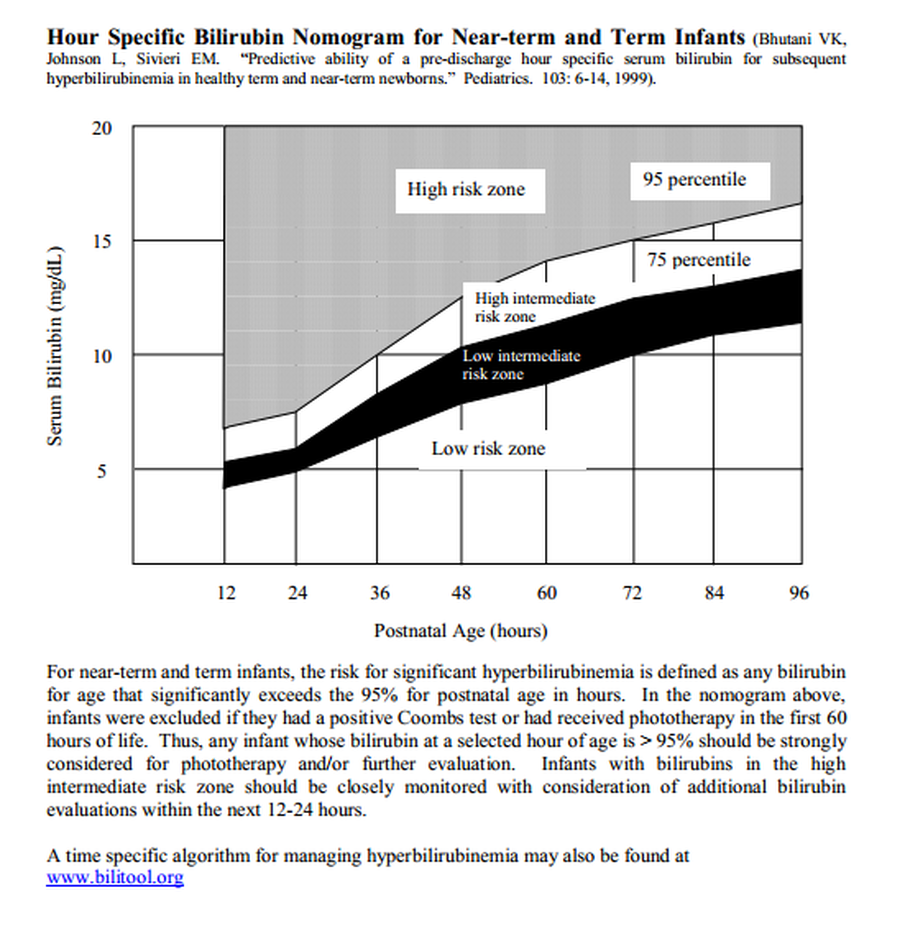
1. Jaundice is more likely to be pathological (vs physiological) when
a. clinical jaundice is noted in the first 24 hrs of life (> 5.0 mg/dL). Mg/dL = mg%
b. serum bilirubin increases more than 5 mg% per day
c. total serum bilirubin exceeds:
- 12-13 mg% in bottle fed term infants
- 15 mg% in breast-fed term infants or
- 8-10 mg% in preterm infants (< 1500 grams)
d. direct bilirubin is > 1.5-2.0 mg% or > 15%-20% of the total bilirubin level
e. jaundice persists > 1 week in term or > 2 weeks in preterm infants.
2. Factors increasing level of physiologic jaundice
a. breast feeding
b. excessive weight loss
c. race - increased in Asians, decreased in African-Americans.
3. Specific factors associated with physiological jaundice
a. shorter RBC half-life leading to greater heme load
b. greater reabsorption of unconjugated bilirubin from the GI tract
c. decreased quantity and activity of bilirubin glucuronyl transferase (responsible for conjugating bilirubin)
B. Pathologic Jaundice
1. Causes
a. overproduction, e.g., hemolytic disease, polycythemia, bruising, IVH.
b. under-conjugation, e.g., inborn errors of metabolism, hypothyroidism, prematurity, breast-milk jaundice.
c. increased reabsorption from the gut (enterohepatic circulation), e.g., ileus, fasting, breastfeeding, GI obstruction.
III. Bilirubin Toxicity
Severe unconjugated hyperbilirubinemia may cause CNS damage - kernicterus. Unfortunately, the exact levels at which the damage may occur are not well defined, in part due to the multifactorial pathophysiology (creating one of the great clinical controversies in Pediatrics). Factors involved include:
A. serum bilirubin level (only free, unbound, indirect bilirubin can cross the blood brain barrier - there are currently no simple, inexpensive tests to measure the fraction of unbound indirect bilirubin vs. bound (to albumin and other serum protein carriers) indirect bilirubin)
B. decreased albumin binding
C. altered blood-brain barrier
The risk of kernicterus may be increased by
A. low serum protein concentration
B. asphyxia
C. acidosis
D. prematurity
E. elevated serum free fatty acids - e.g., infants who are cold stressed, hypoglycemic, or receiving intravenous lipids.
F. certain drugs competing for binding sites e.g., salicylates, sulfonamides, some cephalosporins (Ceftriaxone), oxacillin, indomethacin, Sodium benzoate.
IV. Evaluation
Serum bilirubin levels should be determined in any infant with significant jaundice. In a full-term infant this may not be until the infant is obviously yellow. In a very small preterm infant, levels of 5-6 mg% may be clinically significant but not very impressive to the eye.
If the hyperbilirubinemia has reached non-physiological levels, or therapy is being considered, the infant should be evaluated to determine cause and appropriate therapy.
A. History and Physical
1. review prenatal, labor and delivery history
2. review family history - hemolytic disease, previous infants with jaundice
3. feeding pattern and changes in activity (with lethargic infants and a rapid rise in bilirubin + a direct bilirubin component, be suspicious of sepsis).
4. signs of infection, acute or congenital
5. bruising or cephalohematoma
6. hepatosplenomegaly
7. LGA infants, polycythemic infants.
B. Laboratory Tests
1. bilirubin fractionation (direct versus indirect)
2. maternal and infant blood type; infant’s direct Coomb’s test
3. hematocrit and platelet count (thrombocytopenia may indicate sepsis or TORCH infection)
4. blood smear and reticulocyte count (Rh disease causes RBC shearing and deformity, ABO incompatibility generally produces spherical alterations in RBCs).
If phototherapy is being initiated in small preterm infants with relatively low (physiologic) serum bilirubin levels, the complete evaluation is not always necessary.
V. Treatment
A. What
1. Phototherapy - the primary goal of phototherapy is to control/reduce indirect bilirubin levels to prevent exchange transfusion
2. IVIG infusion – appears to benefit isoimmune hemolytic causes of hyperbilirubinemia by binding up precipitating maternal antibody. Recommended dose is 750 – 1000 mg/kg
3. Exchange Transfusion - an effective method for reducing serum bilirubin, as well as treating hemolytic disease. However, the procedure is time consuming, expensive and carries a moderate risk of morbidity.
B. When - because the levels of “potential toxicity” remain so controversial, the following represent only guidelines suggested by a variety of “experts.”
1. Phototherapy
a. phototherapy should be instituted at a bilirubin level that maintains a distance from the “exchange” level (e.g. 5 mg% less than exchange level).
b. phototherapy should be instituted earlier when the infant’s risks are increased by the situations noted above.
c. reasonable serum bilirubin levels to consider phototherapy might be:
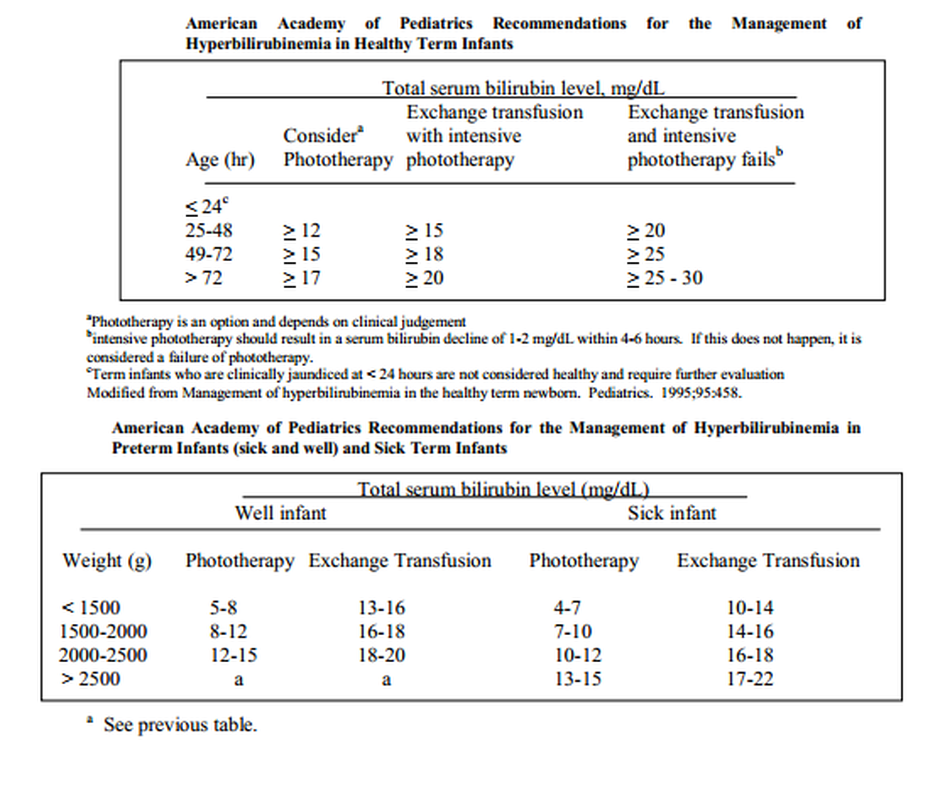
2. Exchange Transfusion
a. many experts feel that a persistent bilirubin level over 20 mg% should be treated with exchange transfusion. In an otherwise healthy, term infant (usually breast fed), bilirubin values > 20 mg% may not need immediate exchange; formula feeding, re-hydration and phototherapy may bring the level down to < 20 mg% in several hours.
b. If the infant is critically ill and/or significantly premature, exchange should be instituted at lower levels or more expediently when critical levels are reached.
c. if hemolytic disease is involved, a rate of rise of bilirubin > 0.5-1.0 mg%/hour may indicate a potential need for exchange transfusion.
d. with the exception of severe hemolytic disease, appropriate phototherapy should prevent most exchange transfusions.
e. exchange transfusions may take many hours for the Blood Bank to prepare. Anticipation of a potential exchange transfusion is crucial. The volume of blood exchanged = 2 times the patient’s total blood volume (90 cc/kg) plus an additional 100 cc to prime the circuit (blood warmer and tubing). Thus, a 3.0 kg infant would need 2 X 90 cc X 3 kg plus 100 cc extra or approximately 640 cc of washed and irradiated blood with a hematocrit of 50% (see exchange transfusion chapter in procedures section of Handbook).
B. How?
1. see exchange transfusion protocol.
2. Phototherapy - requires appropriate light source, intensity and exposure of skin surface area. Results in photoisomerization of the indirect bilirubin molecule leading to enhanced water solubility and greater ability to be excreted by the liver and the kidneys. Appropriate wavelength sought is 450 nanometers. Blue lights should be rated “Special Blue.” We use white lights with a higher intensity that have a significant proportion of 450 nm wavelengths and that are less nausea-producing to the nursing staff than the pure blue lights. The intensity of light only penetrates ~ 1 mm of skin. There is probably no need to shield the gonads of most near term male infants but the eyes of all babies and the gonads of very preterm infants (e.g. <1250 gms) should be shielded.
Complications of & Recommendations for Phototherapy
- insensible water loss increases
- diarrhea is common, increases lactose intolerance
- infant may become lethargic
- due to the above, fluid requirements may increase; infant at risk of dehydration. Monitor closely and in the small infant, consider an arbitrary increase in fluid rate.
- appearance of a “bronze” tint to the skin may indicate that the infant has a significant portion of conjugated bilirubin present (> 2.0 mg%).
- cover the eyes (to avoid potential retinal injury)
- expose the maximum surface area and increase the intensity (add more lights) to enhance bilirubin clearance
- continuous phototherapy is not necessary (thus, brief period out of lights for breast feeding, baths, etc. can be tolerated).
- serum bilirubin levels must be followed. Skin color no longer reflects serum bilirubin levels when an infant is being treated with phototherapy.