RESUSCITATION
I. Who needs resuscitation?
A. Blue baby (+ adequate respiratory effort) and heart rate < 100
1. In the Delivery Room
2. In the Nursery
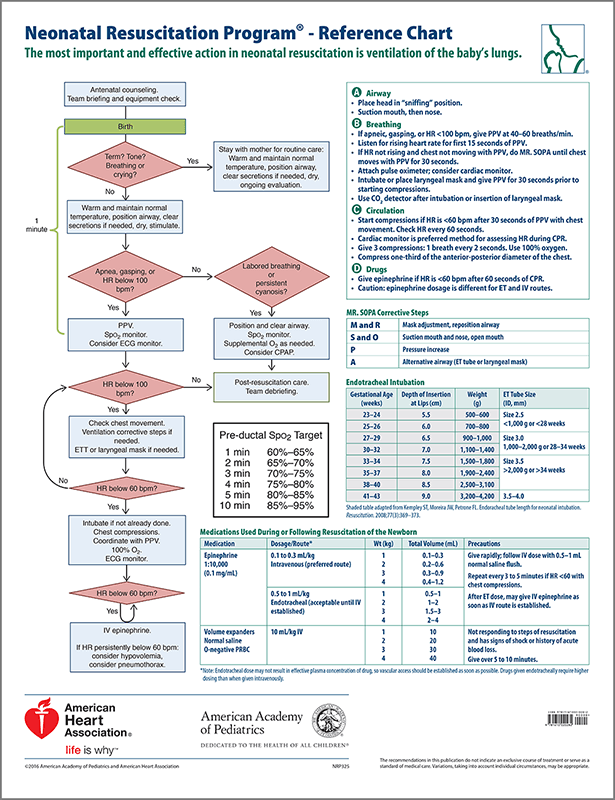
II. Technique of Resuscitation (remember your ABCs!)
A. Clear the airway: this may be performed with bulb suction or a suction catheter. You must have a clear airway in order to ventilate the infant
B. Stimulate the Infant: this may be done by drying the baby with a towel, rubbing the baby’s back, arms and legs or gently suctioning the nose and mouth.
Vigorous or prolonged suctioning with a catheter is potentially dangerous and may lead to a severe bradycardia.
Update for 2015: Infants delivered with meconium stained fluid do not require routine intubation and suctioning. If after appropriate resuscitative efforts have been attempted and the patients HR and respiratory status are not improving tracheal suctioning may be performed.
C. Ventilate the Baby
1. The baby may be ventilated by Neopuff, bag and mask, or via the ETT
2. The Neopuff is almost always adequate for resuscitation and may be used initially in the Delivery Room with four possible exceptions:
a. babies with thick meconium staining (where prolonged bagging may set the stage for severe MAS or pneumothorax).
b. babies with a scaphoid abdomen (known or suspicious for diaphragmatic hernia) where bag-mask ventilation fills the stomach and intestines within the chest cavity with air.
c. infants < 1000 grams birthweight (prolonged continuation of bag-mask ventilation should be limited in this scenario because of the very floppy jaw of these infants, the inability to maintain a tight fit with the mask, and the high likelihood of poorly compliant lung disease.)
d. Severely depressed infant with an Apgar score < 3. Bag-mask ventilation should be done only while the ETT and laryngoscope are being prepared.
3. Do not attempt to intubate an infant without having practiced in a supervised setting with an anesthetized animal model or a mannequin. Do not hesitate to call for help in such a situation. Bag-mask ventilation is appropriate until such assistance arrives.
4. The initial ventilation rate should be 40-60 breaths per minute
5. Watch for chest excursion, increasing HR and “pinking-up” of the baby during bagging.
NOTE: Neopuff needs to be set up properly before use
1. Make sure that you know where the O2 blender control is located.
2. Make sure PIP is set to 20 and PEEP is set to 5.
3. If adequate chest risk is not achieved despite good positioning and proper mask fitting AND if you are positive that an ETT is in good position with PIP of 20 it can be gradually increased.
D. Give cardiac massage
You should begin cardiac massage if the initial heart rate is < 60 bpm despite adequate ventilation with oxygen via ETT for 30 seconds. The manual compression rate should be 90 bpm coordinated with 30 breaths per minute for a total of 120 “events” per minute. Use the wrap-around thumb technique whenever possible (press inward 1/2 to 3/4 of an inch, lower 1/3 of sternum).
E. Give medications: see attached flow sheet.
However, medications are usually not required with proper airway management. If things are not going well, check the ETT position and ventilation parameters (is the oxygen on, is the patient’s chest moving, etc).
The ETT is appropriate route for Epinephrine or Narcan only.
NEVER give NaHCO3 down the ET tube.
Umbilical venous catheter “crash” sets are available in the delivery room - catheter, blade, and umbilical tape. These are meant for rapid insertion following a rapid sterile prep with Betadine, alcohol or chlorhexidine. If long-term central line placement is needed in the NICU, this line should be replaced once the patient is in the NICU. These emergency UVC catheters should only be inserted 4-5 cm (sometimes less in very small infants) just until there is blood return from the catheter.
F. General Principles:
AIRWAY! AIRWAY!! AIRWAY!!! Almost all neonatal resuscitations can be successful if proper airway management and ventilation strategies are use.
1. Remember to continually evaluate response to resuscitation measures. If HR is not increasing and color is not improving, adjust therapy accordingly, i.e., if color is not improving, consider increasing blended oxygen support or if the infant is intubated, is the ETT in correct position? Is ETT plugged with secretions? Is there a pneumothorax? If HR is still not coming up and airway patency and ventilation are confirmed, consider IV fluid volume and/or drugs.
2. Always ask for help; one person cannot resuscitate a baby single-handedly.
3. One person should always be designated “the leader,” i.e., the senior most Resident or - if a senior Resident is absent - an NNP, and he/she should assign duties to the other personnel present.
4. If aggressive resuscitative measures are anticipated, draw up medications and/or fluid volume in advance, check equipment and call for extra hands.
5. Use the transport incubator for the trip from the Delivery Room to the NICU.
Always resuscitate infants in the Delivery Room (i.e., never run with a baby from the DR to the NICU!)
Never remove an infant requiring supplemental oxygen from the oxygen source on the trip from the Delivery Room to the NICU (ie, use the transport incubator and its oxygen supply).
G. Consider the following in any infant requiring significant resuscitation:
1. Cardio-respiratory monitoring for at least 12-24 hours
2. Blood pressure monitored via direct continuous arterial pressure readout or at least q 1 hr until normal.
3. Blood sugar screening test q 1 hr X 3 even if IV fluid access is established. Maintain 4-8 mg/kg/min of glucose intake with IVF.
4. Arterial or capillary blood gas if any abnormal vital signs or cyanosis.
5. If receiving oxygen, follow the saturations and the trend of FIO2 requirement.
6. If NPO, IV fluids restricted to insensible losses plus volume of urine output until urine output is normal (because of risk of acute renal injury).
7. Urine checked for blood, glucose and protein
8. Urine volume measured
9. Feedings delayed or introduced with caution
10. Weigh daily
11. Bath delayed until vital signs stable at least 6 hours.
12. Tone, reflexes and wake/sleep state noted every hour
I. Who needs resuscitation?
A. Blue baby (+ adequate respiratory effort) and heart rate < 100
1. In the Delivery Room
2. In the Nursery
II. Technique of Resuscitation (remember your ABCs!)
A. Clear the airway: this may be performed with bulb suction or a suction catheter. You must have a clear airway in order to ventilate the infant
B. Stimulate the Infant: this may be done by drying the baby with a towel, rubbing the baby’s back, arms and legs or gently suctioning the nose and mouth.
Vigorous or prolonged suctioning with a catheter is potentially dangerous and may lead to a severe bradycardia.
Update for 2015: Infants delivered with meconium stained fluid do not require routine intubation and suctioning. If after appropriate resuscitative efforts have been attempted and the patients HR and respiratory status are not improving tracheal suctioning may be performed.
C. Ventilate the Baby
1. The baby may be ventilated by Neopuff, bag and mask, or via the ETT
2. The Neopuff is almost always adequate for resuscitation and may be used initially in the Delivery Room with four possible exceptions:
a. babies with thick meconium staining (where prolonged bagging may set the stage for severe MAS or pneumothorax).
b. babies with a scaphoid abdomen (known or suspicious for diaphragmatic hernia) where bag-mask ventilation fills the stomach and intestines within the chest cavity with air.
c. infants < 1000 grams birthweight (prolonged continuation of bag-mask ventilation should be limited in this scenario because of the very floppy jaw of these infants, the inability to maintain a tight fit with the mask, and the high likelihood of poorly compliant lung disease.)
d. Severely depressed infant with an Apgar score < 3. Bag-mask ventilation should be done only while the ETT and laryngoscope are being prepared.
3. Do not attempt to intubate an infant without having practiced in a supervised setting with an anesthetized animal model or a mannequin. Do not hesitate to call for help in such a situation. Bag-mask ventilation is appropriate until such assistance arrives.
4. The initial ventilation rate should be 40-60 breaths per minute
5. Watch for chest excursion, increasing HR and “pinking-up” of the baby during bagging.
NOTE: Neopuff needs to be set up properly before use
1. Make sure that you know where the O2 blender control is located.
2. Make sure PIP is set to 20 and PEEP is set to 5.
3. If adequate chest risk is not achieved despite good positioning and proper mask fitting AND if you are positive that an ETT is in good position with PIP of 20 it can be gradually increased.
D. Give cardiac massage
You should begin cardiac massage if the initial heart rate is < 60 bpm despite adequate ventilation with oxygen via ETT for 30 seconds. The manual compression rate should be 90 bpm coordinated with 30 breaths per minute for a total of 120 “events” per minute. Use the wrap-around thumb technique whenever possible (press inward 1/2 to 3/4 of an inch, lower 1/3 of sternum).
E. Give medications: see attached flow sheet.
However, medications are usually not required with proper airway management. If things are not going well, check the ETT position and ventilation parameters (is the oxygen on, is the patient’s chest moving, etc).
The ETT is appropriate route for Epinephrine or Narcan only.
NEVER give NaHCO3 down the ET tube.
Umbilical venous catheter “crash” sets are available in the delivery room - catheter, blade, and umbilical tape. These are meant for rapid insertion following a rapid sterile prep with Betadine, alcohol or chlorhexidine. If long-term central line placement is needed in the NICU, this line should be replaced once the patient is in the NICU. These emergency UVC catheters should only be inserted 4-5 cm (sometimes less in very small infants) just until there is blood return from the catheter.
F. General Principles:
AIRWAY! AIRWAY!! AIRWAY!!! Almost all neonatal resuscitations can be successful if proper airway management and ventilation strategies are use.
1. Remember to continually evaluate response to resuscitation measures. If HR is not increasing and color is not improving, adjust therapy accordingly, i.e., if color is not improving, consider increasing blended oxygen support or if the infant is intubated, is the ETT in correct position? Is ETT plugged with secretions? Is there a pneumothorax? If HR is still not coming up and airway patency and ventilation are confirmed, consider IV fluid volume and/or drugs.
2. Always ask for help; one person cannot resuscitate a baby single-handedly.
3. One person should always be designated “the leader,” i.e., the senior most Resident or - if a senior Resident is absent - an NNP, and he/she should assign duties to the other personnel present.
4. If aggressive resuscitative measures are anticipated, draw up medications and/or fluid volume in advance, check equipment and call for extra hands.
5. Use the transport incubator for the trip from the Delivery Room to the NICU.
Always resuscitate infants in the Delivery Room (i.e., never run with a baby from the DR to the NICU!)
Never remove an infant requiring supplemental oxygen from the oxygen source on the trip from the Delivery Room to the NICU (ie, use the transport incubator and its oxygen supply).
G. Consider the following in any infant requiring significant resuscitation:
1. Cardio-respiratory monitoring for at least 12-24 hours
2. Blood pressure monitored via direct continuous arterial pressure readout or at least q 1 hr until normal.
3. Blood sugar screening test q 1 hr X 3 even if IV fluid access is established. Maintain 4-8 mg/kg/min of glucose intake with IVF.
4. Arterial or capillary blood gas if any abnormal vital signs or cyanosis.
5. If receiving oxygen, follow the saturations and the trend of FIO2 requirement.
6. If NPO, IV fluids restricted to insensible losses plus volume of urine output until urine output is normal (because of risk of acute renal injury).
7. Urine checked for blood, glucose and protein
8. Urine volume measured
9. Feedings delayed or introduced with caution
10. Weigh daily
11. Bath delayed until vital signs stable at least 6 hours.
12. Tone, reflexes and wake/sleep state noted every hour