|
Key Principles:
|
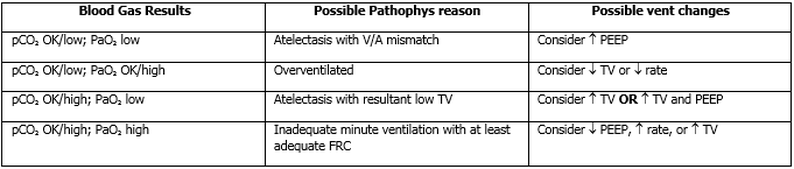
In order to effectively manage the respiratory status of a patient, one must be able to use the ventilator to alter the pO2 & pCO2. Oxygenation, pO2, is determined by the MAP & FiO2. Ventilation, pCO2, is determined by minute ventilation, the rate x Vt (tidal volume).
|
|
Nasal Continuous positive airway pressure (CPAP)
|
Provides PEEP to maintain FRC in babies who have weaned from the conventional vent or don’t yet need to be intubated.
|
|
Conventional Ventilator
|
Currently, the NICU utilizes 2 modes conventional ventilation:
1. Pressure Control/Assist Control with Volume Guarantee - ventilator determine pressure necessary to generate the ordered tidal volume. 2. Pressure control SIMV- Inspiratory pressures are adjusted to affect Vt. P support function as a weaning mechanism and is usually 1/2-2/3 inspiration pressure. |
- Give FiO2 to achieve desired saturations of:
- 87-95% with goal saturation of 90% if FiO2 ≥ 40% on CPAP or ventilator
- 87-95% with goal saturation of 92% if FiO2 ≤ 40% on CPAP, HFNC, or ventilator
- Start with rate of 30-40
- Start with initial tidal volume of 5 – 6 ml/kg for preterm infants and 4 – 5 ml/kg for term infants.
- Target ABG’s are pH 7.25-7.35; pCO2 45-55, pO2 60-90
Initial Ventilator Settings
- Remember to wean FiO2 to maintain O2 sats in goal range
- TV of 4.5-6.5 ml/kg
- Write the order in the chart for the desired TV and take note of initial peak pressures (PIP)
- Adjust based on chest expansion, air entry and blood gasses
- PEEP of 5-6 cm H2O
- Rate of 30-40 bpm
Example Settings – what to order
- Drager PC/AC: TV=5.5ml/kg, PEEP=6, Rate=40
Bronchopulmonary Dysplasia
- Note that management varies with each baby
- General Goals: pH>7.25, pCO2 50-60, and pO2>60 or O2 sat 92-96%.
- Avoid desaturation with feedings, suctioning, agitation
General Vent Management Guidelines
- Should be used for preterm infants less than 7 days of age with RDS
- Incorporate findings on exam, CXR, trends of minute ventilation & tidal volumes
- Weaning the rate on PC-AC or PC-PSV does not affect the baby’s ventilation if they are consistently breathing over the set ventilator rate, however decreasing the rate is appropriate to ensure the patient does not have significant apnea prior to extubation.
- Once an adequate tidal volume is determined the Vt should not have to be weaned, the baby will self-wean peak pressure (PIP) as compliance of the lungs improves.
- Appearance of respiratory distress, hypoxemia, hypercarbia are indications to halt further weaning
|
High Frequency Oscillator Ventilation
(HFOV) |
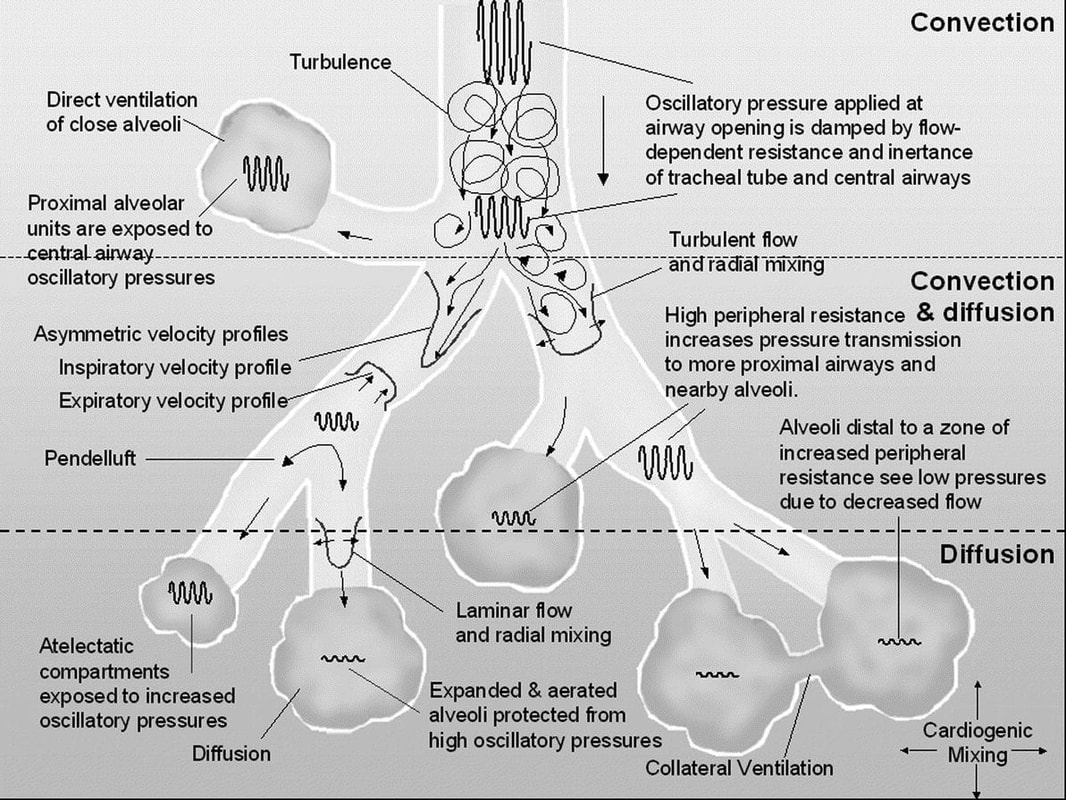
Pulses or oscillates gases at a frequency of 120-1500 times per minute. Oscillations are generated by a to-and-fro movement of a piston. On inspiration a column of gas is pushed into the airway. During exhalation gas is drawn out of the airway. Both inspiration and expiration are active.
|
- Start at a MAP that is 20-30% higher than the MAP on the conventional ventilator
- Increase the MAP repeatedly in increments of 1-2 cmH2O until adequate oxygenation is achieved
- Keep MAP at the optimal value until are able to decrease the FiO2 <60%
- Obtain CXR soon after initiating HFOV to evaluate for hyperinflation
- Baseline lung volume goal = 7 - 8 rib expansion
- Flattening of diaphragms will be seen if hyperinflation
- If signs of over-inflation, decrease MAP by 1-2 cm H2O and re-evaluate
- Follow-up CXR in 2-4 hours after changes made in MAP
- Baseline lung volume goal = 7 - 8 rib expansion
- Start DP at 10-15 cm H2O higher than PIP on CMV
- Watch chest movement to assure adequate chest wiggle
- Increase DP by 2-4 cm H2O increments
- If maximum DP is reached and PaCO2 is still high, decrease frequency in order to decrease PaCO2
- Freqency (Hz) guidelines:
- 10-12 Hz for birthweight between 2-5 kg
- Obtain blood gas ~20-30 minutes after the patient has been stable on HFOV
- Reduce FiO2 to <40% before weaning MAP
- Exceptions:
- over-inflation
- air leak syndromes where decreasing MAP takes priority over decreasing FiO2
- over-inflation
- Reduce MAP in 1-2cm increments to 8-9
- Wean amplitude (DP) in 2-4cm increments
- Don’t wean the frequency
SURFACTANT and RDS
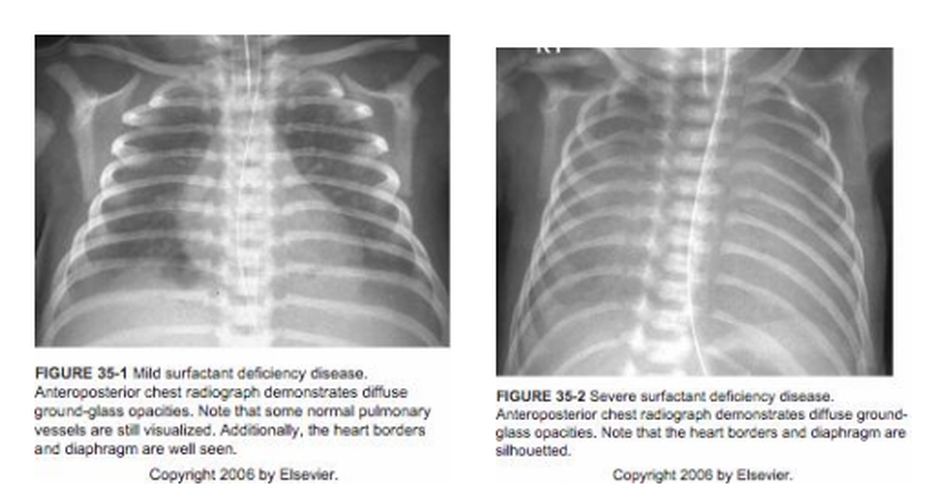
Premature infants are at high risk for surfactant deficiency secondary to decreased numbers of alveoli, decreased numbers of functional Type II pneumocytes and decreased phospholipid storage pools. Nevertheless, surfactant deficiency is not an all-or-none phenomenon and its presence in sufficient quantities to allow adequate lung expansion and gas exchange varies from infant to infant. Thus, in infants < 28 weeks gestation, approximately 70-80% have the clinical signs and X-ray appearance of RDS. This incidence slowly decreases to approximately 1% of infants at 36 weeks gestation. However, certain groups of near-term and term infants are at risk of surfactant deficient lung disease including infants of diabetic mothers (fetal insulin antagonizes surfactant protein production and phospholipid production), asphyxiated infants, septic infants and infants who have aspirated blood, amniotic fluid, meconium or feedings.
Natural surfactant production is heavily influenced by hormonal changes in the developing fetus. The two principle hormones which dramatically increase fetal surfactant production and lung maturation are corticosteroids and thyroxine. The American College of Obstetrics & Gynecology (ACOG) has thus recommended that all women < 34 weeks EGA receive antenatal steroids if in imminent danger of delivery (exception: maternal or fetal infection). There is considerable debate about whether subsequent rounds of steroid therapy have any merit in at-risk preterm mothers.
The normal surfactant content of term infants is 100 mg/kg of body weight. At GHS, we have chosen to use a “natural surfactant” derived from lung lavage washings from newborn calves. This commercially available product is known as Infasurf (marketed by Forest Laboratories). However, it differs from human surfactant in several ways. Human surfactant is comprised of several Surfactant proteins, several different phospholipids (primarily dipalmytyl-phosphatidylcholine, DPPC) and neutral lipids. Infasurf has no surfactant protein A (responsible for surfactant re-uptake and re-processing) or other hydrophilic compounds, which are lost in the pharmaceutical extraction process and thus, have proven beneficial but only in a limited fashion (i.e., decreased mortality and air leak but no overall change in BPD or length of stay). Currently, there is overwhelming statistical evidence demonstrating that surfactant use decreases both mortality and the number of air leaks associated with RDS. Surfactants have also been shown to decrease morbidity associated with other, surfactant-deficient diseases that may occur in more mature neonates such as meconium aspiration syndrome or sepsis with pulmonary involvement. During the acute phase following surfactant administration, there is also less need for high MAP and high FIO2.
No significant reproducible side effects have been noted following surfactant administration. Transient desaturations may occur during the period of administration.
- Initial Dose: should be given as soon as possible to any preterm infant (< 36 weeks EGA) if:
- In the delivery room to any infant < 26 weeks EGA (prophylactic dosing) or any other preterm infant in the DR with clear clinical evidence of RDS.
- In the NICU, < 36 weeks EGA, on > 40% oxygen, and with suspected RDS. Administer Infasurf prior to the application of positive pressure (ventilation or CPAP).
- In the NICU a term infant is having respiratory distress due to surfactant inhibition (e.g. Meconium Aspiration or pneumonia), is requiring mechanical ventilation or CPAP and has a compatible CXR for aspiration syndrome or severe pneumonia.
- In the delivery room to any infant < 26 weeks EGA (prophylactic dosing) or any other preterm infant in the DR with clear clinical evidence of RDS.
- Initial Dose: should be given (or strongly considered) as soon as possible if:
- known diaphragmatic hernia exists and subsequent respiratory distress compromise ensues (the relative lung hypoplasia of these infants is associated with a profound surfactant deficiency).
- older near term infants with a clinical presentation and CXR consistent with surfactant deficiency (e.g. pneumonia, other sepsis, meconium aspiration syndrome)
- Subsequent doses may be repeated q 8 - 12 hours if infant still requires intubation, has an FIO2 > 30% and has a PaO2 < 80 mm Hg.
- Technique and Complications
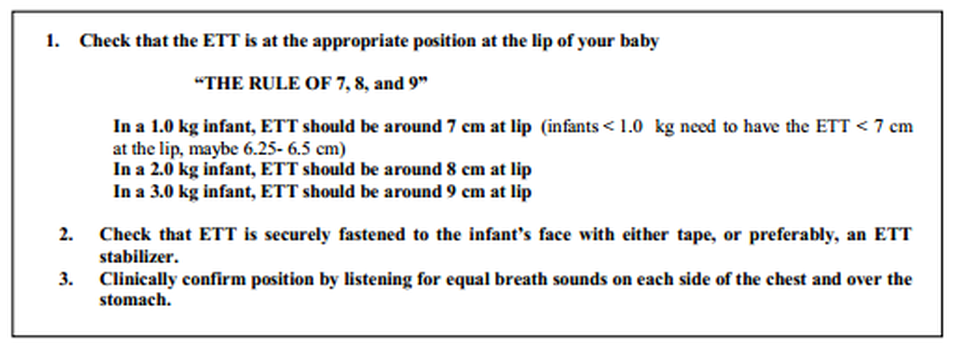
- Given by the Respiratory Therapists via the endotracheal tube. Infant is rotated between 2 alternate positions to optimize distribution. Each dose = 105 mg/kg or 3 mL/kg. You should avoid suctioning the infant for 2 hours after each dose.
- Tube plugging: this very viscous substance may occlude ETT if ventilatory pressures are not sufficiently high. May require brief bagging to push surfactant downstream. One should not rotate infant’s position for next dose until oxygen saturations are > 88%.
- Bradycardia: a hypervagal response is reported ~ 8% of the time. There are very rare reports of fatal asystole. Watch vital signs closely during the administration of surfactant
- Pneumothorax: probably related to dramatic changes in lung compliance following surfactant introduction. Infants on very high airway pressures should have their pressures diligently decreased following surfactant administration (can use O2 sats, PaO2, PaCO2, TCOM).
|
Nasal Cannula Oxygen
|
- Long-term oxygen delivery for neonates with a chronic, stable oxygen requirement of less than 25-150 mL/min. A flow rate > 200-250 mL/min requires attending approval.
- Oxygen administration for patients with a stable oxygen requirement who would benefit from developmental interactions and p.o. feeds.
- Delivery of oxygen via nasal cannula is not indicated in acute disease (e.g., the first few days after birth, in the immediate period after extubation, with increasing respiratory distress, or with increasing O2 requirement over a 24 hour period.)
- Administration of oxygen via nasal cannula is contraindicated for neonates that require a stable delivery system. The FiO2 that is delivered may fluctuate with respiratory rate, tidal volume, respiratory effort and patency of the nasal airway.
- High flow rates of unwarmed, non-humidified O2 may damage nasopharyngeal mucosae. All nasal cannula delivery systems should include a bubble humidifier. Again, any flow rate > 200-250 mL/min requires attending approval.