NEONATAL HYPOGLYCEMIA
I. Infants at Risk for Hypoglycemia
A. Infants of diabetic mothers
B. Large for gestational age infants
C. Small for gestational age infants
D. Preterm infants
E. Sick or stressed infants
F. Unintentional discontinuation of IV infusion
G. Polycythemia
H. Infants on return from OR especially if they have not received any dextrose during surgery.
All infants at risk for hypoglycemia must be monitored with frequent glucoses (serum glucose values are more clinically significant and accurate than whole blood glucoses – but only if glucose oxidase electrodes are used) .
II. Symptoms of Hypoglycemia
A. None (asymptomatic)
B. Jitteriness
C. Tremors
D. Seizures
E. Lethargy
F. Apnea
G. Cyanosis
H. Respiratory distress
III. Definition of Hypoglycemia - another controversial subject in Neonatology!
A. Dextrostix < 25-45 mg% (confirm low value with serum glucose determination).
B. Serum glucose < 30-40 mg%.
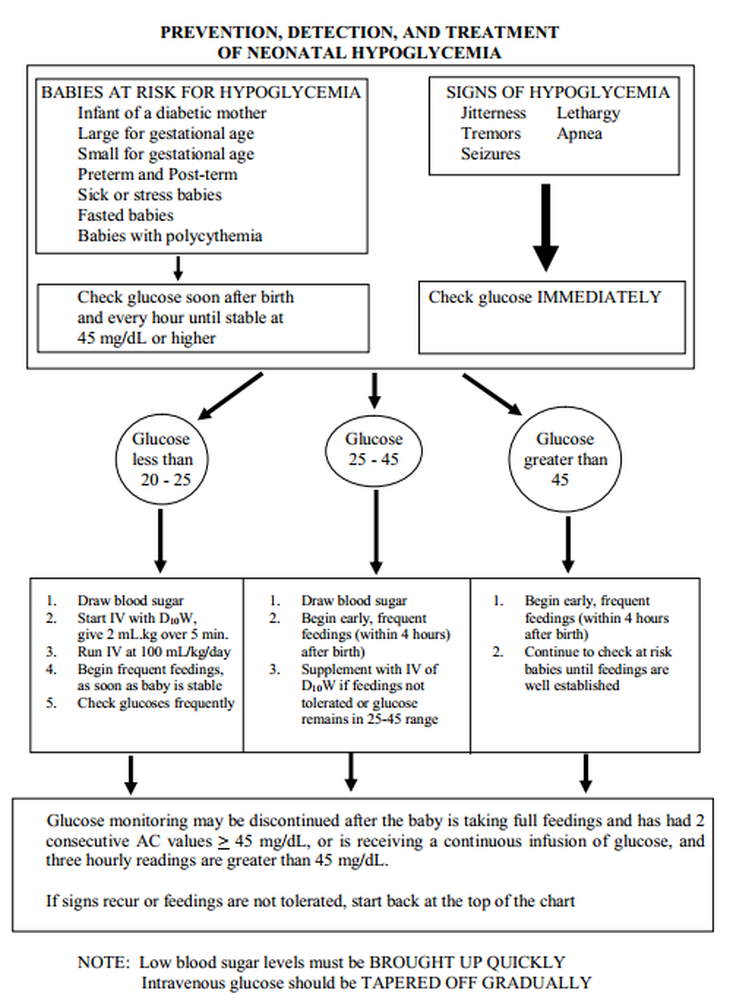
IV. Treatment of Hypoglycemia in the NICU
A. Infants at Risk who are normoglycemic
1. Stable near term or term infants: start feeding at 2-4 hours of age. Use enteral D5W if the baby is unable to tolerate nipple feedings. If baby is unable to tolerate any feedings, begin an IV infusion with 10% glucose at 6-8 mg/kg/min.
2. Unstable Newborns or otherwise sick infants: begin an IV infusion with 10% glucose.
B. Infants who have developed hypoglycemia (ie, BG < 40 mg/dL):
1. Immediately:
a. If an infant is stable and able to start enteral feedings and the initial blood glucose < 40 mg/dL, you may feed 20-30 mL of formula and check postprandial glucose level. If postprandial glucose is > 45 mg/dL, then you may continue to check AC glucoses until 2 consecutive BG values exceed 45 mg/dL.
b. if an infant is stable with an IV in place (but unable to begin enteral feedings) and the BG is between 35-40 mg/dL, it is acceptable to begin maintenance IVF at 80-100 cc/kg/day using D10 to D12..5. Blood glucoses should be repeated in one hour or less after starting IVF in this scenario.
c. If an infant is unstable or symptomatic, give 200 - 300 mg/kg of glucose (2 - 3 cc/kg of D10W) over 1-2 min. This dose may need to be repeated. However, a large bolus (> 3 cc/kg of D10W) should not be given – especially in IDM infants - as this may cause a sudden insulin pulse from the infant’s hypertrophied pancreas and actually exacerbate the problem.
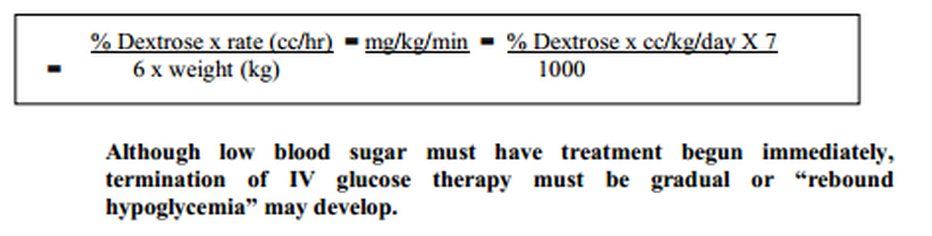
2. Maintenance - follow above by continuous infusion of 10% glucose at a rate of 6-8 mg/kg/min until glucose values stabilize in the normal range. Increase rate and/or glucose concentration as needed to keep values normal. NOTE: 8 mg/kg/min = 120 cc/kg/day of D10). As feedings are tolerated, the infusion should be tapered gradually as blood glucose readings are checked frequently. However, the infusion may be required for 24-48 hours or longer.
A quick formula to calculate glucose infusion rate (in mg/kg/min)
C. Refractory hypoglycemia (hypoglycemia persisting despite administration of 15 mg/kg/min of IV glucose) - consider IV hydrocortisone (5 mg/kg dose q 12 hours IV, IM, or PO) or oral diaxozide (a thiazide derivative that can decrease insulin secretion and increase catecholamine release), and consider an Endocrine consult (Hint: to please your Endocrine consultant, if blood glucose < 40 mg%, draw a serum free cortisol, insulin, C-peptide -which is cleaved off the pre-insulin molecule - and growth hormone levels before starting steroids or diaxozide). Alternative pharmacological treatments that require endocrine consultation include glucagon and epinephrine (benefits are very transient), and somatostatin (a neuropeptide that inhibits release of glucagon, insulin, GH and thyrotropin).
Diazoxide is currently the most commonly used drug in the hyperinsulinemic infant who is able to tolerate enteral feeds, 5-20 mg/kg/day orally Q 8 - 12 hours.
D. Helpful hints for treatment of hypoglycemia:
1. After beginning IV glucose therapy, frequently check placement and flow of baby’s IV
2. Even if baby is receiving treatment for hypoglycemia, Dextrostix values or blood sugar levels must be checked frequently. This is done to assure that infant is receiving adequate glucose.
3. See flow chart on next page.
When bringing blood sugar levels up quickly, do NOT use very concentrated sugar solutions such as 25%-50% glucose. Highly concentrated (hyperosmotic) glucose solutions may cause cerebral damage in small infants.